(1)
Marina Spine Center, Marina del Rey, CA, USA
Use the standard thoracotomy approach for safe exposure of vertebral levels T2–L2. Proper rib selection depends on the pathology for most cases, especially those involving a strut graft. The rib to resect for a certain vertebral level is chosen by one of two methods:
1.
When the pathology dictates a direct anterior approach to the vertebral column, that is, kyphotic TB abscess, choose the rib directly horizontal to the vertebral level at the midaxillary line in an anteroposterior (AP) chest X–ray. The rib removed must be cephalad to the lesion to give adequate proximal exposure while working down the lesion [1].
2.
When direct access to the spinal canal is needed at one disc, that is, a thoracic disc excision, resect the rib that leads to that disc, that is, 9th rib to the T8–T9 disc.
There are anatomical variations at the cervicothoracic and thoracolumbar junctions that dictate the rib to be taken. For patients with a large abscess in the right chest or in other circumstances that dictate a right thoracic approach, be prepared to mobilize the vena cava and associated veins from that side.
Get Clinical Tree app for offline access

1.
Place the patient in the lateral decnbitus position. Approach from the left side, as it is much easier to handle, the aorta and the segmental vessels from the left side.
With the patient in a supine position, insert a double-branched endotracheal tube into the right and left mainstcm bronchi to allow selective collapse of the left lung. A standard endotracheal tube may also be used. When the left chest is chosen for the approach, place the patient in the right lateral decubitus position. Center the midthorax of the patient over the break in the table. Pad well under the dependent axilla; pad and protect the left arm. Stabilize the pelvis with a strap to the table, place a pillow between the legs, and pad all bony prominences.
2.
Open the skin and subcutaneous tissue from the lateral border of the paraspinous musculature to the sternocostal junction over the rib to be resected. Placing the thoracotomy incision slightly tangential to the rib to be resected allows easier resection of more than one rib if necessary (Fig. 17.1).
Fig. 17.1
Using the lateral decubitus position, make the standard thoracotomy skin incision over the rib to be resected. The rib to resect for a vertebral level is usually the rib directly horizontal to the vertebral level at the midaxillary line in an anteroposterior (AP) chest X–ray. The approach is cephalad to the lesion, as it is better to resect a rib that allows one to work down on the lesion rather than a more distal rib, which would necessitate working up to the lesion. For scoliosis, the approach is from the convexity of the lesion, and for non-scoliotic conditions the approach from the left side is preferred. Open the skin of subcutaneous tissue from the lateral border of the paraspinous musculature to the sternocostal junction over the rib to be resected. Placing the thoracotomy incision slightly tangential to the rib to be resected allows easier resection of more than one rib if necessary
Insert self-retaining retractors and extend the wound with electrocautery down through the muscle layers of the thorax. When needed for full exposure, section the latissimus dorsi, trapezius, and rhomboid major and minor muscles.
3.
After exposure of the chest wall (Fig. 17.2), count the ribs from the 12th up to the appropriate rib or from the 1st rib downward. The 1st rib appears to be inside the 2nd when one is palpating from this angle and it is often difficult to find. Each rib articulates with the superior portion of the body in the area of the disc space of the level above. Therefore, the 12th rib inserts closer to the T11–T12 intervertebral disc space. X-ray confirmation can be obtained if necessary.
Fig. 17.2
Using electrocautery, cut directly to the outer periosteum of the rib through any intervening muscle or subcutaneous tissue. Obtain adequate hemostasis
4.
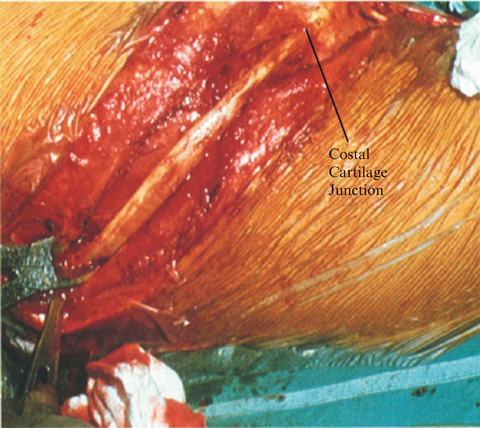
Expose the outer periosteum of the rib with the electrocautery and cut directly to bone through the periosteum from the angle of the rib to the costal cartilage (Fig. 17.3). Elevate the periosteum off the outer rib surface (Fig. 17.4). Use the curved-tip rib elevator to strip the superior and inferior borders of the rib, maintaining an intact elevated periosteum, and use the Doyen to elevate the inner periosteum of the under-surface of the rib (Fig. 17.5).
Fig. 17.3
Cut directly to bone through the outer periosteum of the rib with electrocautery
Fig. 17.4
Using the periosteal elevator, elevate the periosteum first from the outer surface of the rib, then the superior surface, followed by the inferior surface of the rib
Fig. 17.5
Using the Doyen elevator, remove the periosteum from the undersurface of the rib
Caution: Avoid damaging the intercostal vessels that course on the inferior surface of the rib. Elevate the periosteum of the rib by cutting with the elevator directly on bone. Avoid plunges that might inadvertently enter the pleura.
5.
With the intact periosteum freed from the rib, cut the rib with the rib cutter as far posteriorly as necessary between the costotransverse joint and the angle of the rib, and anteriorly at the costal junction (Fig. 17.6). Remove the rib and save it for bone graft. Bone wax the end of the rib lightly after rasping to make sure there are no ragged edges. Tie a sponge on the tip of the stump for protection to the surgeon during the procedure.
 Cervicothoracic Junction
Cervicothoracic Junction
 Supraclavicular Approach
Supraclavicular Approach
 Anterior Lateral Approach to the Upper Cervical Spine
Anterior Lateral Approach to the Upper Cervical Spine
 Microcervical Foraminotomy: An Alternative Posterior Technique for Intractable Radicular Pain
Microcervical Foraminotomy: An Alternative Posterior Technique for Intractable Radicular Pain
 Lumbar Laminotomy, Foraminotomy, Root Decompression, and Discectomy in the Lateral Position
Lumbar Laminotomy, Foraminotomy, Root Decompression, and Discectomy in the Lateral Position
 Posterolateral Foraminal Approach to the Lumbar Disc
Posterolateral Foraminal Approach to the Lumbar Disc




Related posts:
Cervicothoracic Junction
Supraclavicular Approach
Anterior Lateral Approach to the Upper Cervical Spine
Microcervical Foraminotomy: An Alternative Posterior Technique for Intractable Radicular Pain
Lumbar Laminotomy, Foraminotomy, Root Decompression, and Discectomy in the Lateral Position
Posterolateral Foraminal Approach to the Lumbar Disc
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree