Chapter 23 Total Spondylectomy for Subaxial Cervical Spine Tumors
INTRODUCTION
Subaxial cervical tumors are relatively uncommon compared with those involving the thoracic and lumbar regions, and represent less than 10% of spinal metastases.1 The surgical treatment of these tumors is often complicated by functional nerve root and brachial plexus involvement, vertebral artery (VA) encasement, and the need for multilevel reconstruction after anterior-posterior decompression.
PREOPERATIVE ASSESSMENT
RADIOLOGICAL ASSESSMENT
NEUROLOGICAL ASSESSMENT
POSTERIOR APPROACH (FOR C5–7 LESIONS)2
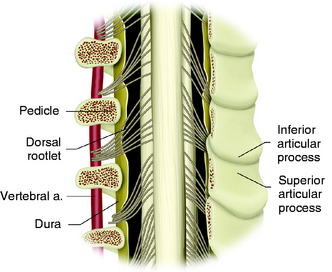
The patient is placed in a prone position with skeletal fixation. A midline skin incision is made from C2 to T4 and a paraspinal muscle dissection is performed (Fig. 23-1). Wide exposure is necessary to access the lateral margin of the facet joints. Total laminectomies are performed from C5 to C7, and bilateral facetectomies are completed at C4–5, C5–6, and C6–7. The facet removal is made from the spinal canal side to the lateral side. After the facet removal, the C5, C6, and C7 nerve roots are seen and the VA posterior surface is exposed (Fig. 23-2). The posterior bony capsules of the VA are continued through the pedicle to the VB. They are removed with a punch, and the pedicles are drilled away to the VB so that the partial removal of the VB can be attempted via the transpedicular route. When transpedicular VB removal is attempted, the upper roots are retracted to the cephalad direction and the VA is retracted to the lateral side.3 This maneuver provides a wider operative field to the VB.
ANTERIOR APPROACH (C5–7 COMPLETE VERTEBRECTOMY)
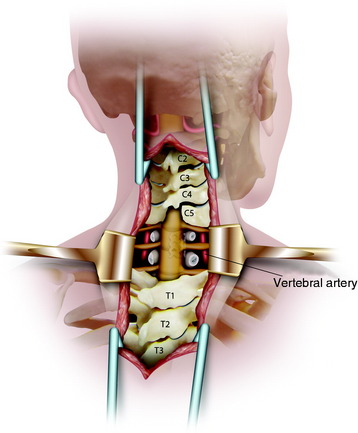
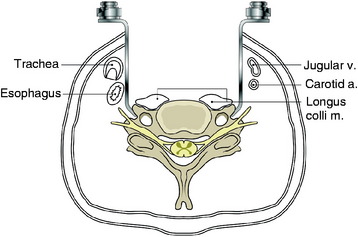
The retractors should be located beside the transverse process along the lateral side of the longus colli muscle (Fig. 23-3). The cephalad retractor is positioned on the C4 transverse process, and the caudal retractor is on the T1 transverse process. In the middle of the field, the self-retractor is laid over the muscles.
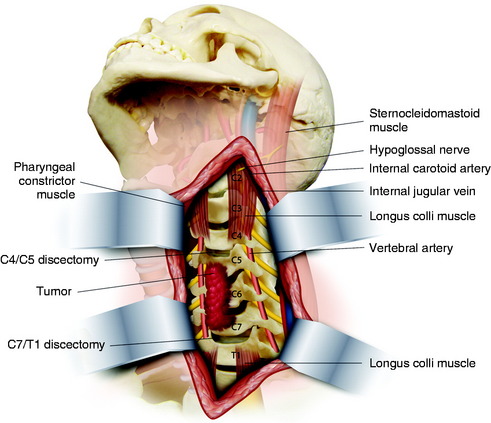
The longus colli muscle should not be dissected on the VB surface. The longus colli muscles are sectioned over the entire width at the C4–5 intervertebral disc level and the C7–T1 intervertebral disc level (Fig. 23-4). The resected segments are swept away from the VB surface. When the muscles are removed at the C7 VB level, the VA is located anterior to the transverse process of C7 and enters the C6 vertebral foramen. Great care should be taken to prevent injury to the VA.
CORPECTOMY
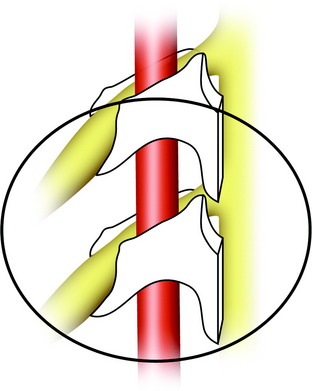
The uncinate processes are identified and used as reference points for establishing the width of the corpectomy required (Fig. 23-5).4 Posterior cortical bone and osteophytes are removed microsurgically with the aid of the microscope. Decompression is considered to be successful when the surgeon can directly visualize a protruding, pulsating dural sac.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


