(1)
Marina Spine Center, Marina del Rey, CA, USA
1.
Preoperative preparation of the patient should include oral and nasal cultures. Preoperative antiseptic gargles and tetracycline, which were used in the past,1 are not needed. No special antibiotic coverage is used for normal oral flora.2 Standard prophylactic antibiotics are used.
2.
After intubation and anesthesia, perform a tracheostomy.1 Insert the short cuff tube. Position the patient supine with the head slightly flexed on occipital pads. A more upright position can be used with certain precautions.
3.
Insert the Boyle-Davis or Mclver ENT retractor to allow depression of the tongue and self-retaining retraction of the mouth. Be certain there is adequate padding for the lips and teeth (Fig. 2.1). Place a collagen sponge into the nasopharynx to control drainage. For adequate visualization of the posterior pharynx, usually the soft palate must be retracted first. Retract the soft palate with soft rubber tubes placed through the nasal cavity and out the oral cavity and tie with adequate padding on the lips (Fig. 2.2).
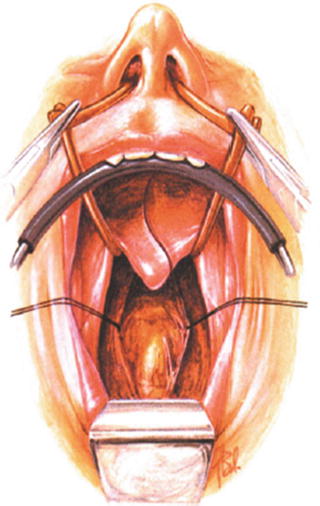
Fig. 2.1
The Boyle-Davis or Mclver ENT retractor is inserted to allow adequate retraction of the tongue. The soft palate may be incised to allow stay suture retraction or retracted with naso-oral soft rubber tubes. The posterior pharynx is opened longitudinally and bluntly dissected transversely to reveal the anterior tubercle of C1
Fig. 2.2
The operative field showing the packing in the hypopharynx and the exposed posterior pharyngeal wall
4.




If adequate soft palate retraction is not obtained, the soft palate is incised in a curvilinear incision around the uvula and the cut edges are retracted with stay sutures to the lateral walls of the oropharynx.1,3
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
