| 87 | Transoral Approach/Decompression |
♦ Preoperative
Imaging
- Magnetic resonance imaging to assess brain stem or spinal cord compression
- Plain x-rays in traction to determine the extent of reduction
- Computed tomography to assess the vertebral artery at C2 for posterior fusion planning
Preoperative Care
- Patients with degenerative ventral compressive lesions or basilar invagination are admitted preoperatively and placed in traction. If the patient–s symptoms improve with reduction, treat with posterior fusion only.
- Start with 5 pounds of traction and slowly increase to a maximum of 15 pounds. Make sure the vector of traction is neutral or with slight extension. Obtain lateral x-ray films after each change in weight.
Equipment
- Self retaining transoral retraction system and table cross-bar attachment
Operating Room Set-up
- Somatosensory and motor evoked potential monitoring (optional)
- Fluoroscopy
- Balanced microscope
- Image guidance
- Supine on operating table
- Head fixed in Mayfield head holder in slight extension
- Attach self retaining transoral retractor to table.
- Tongue and endotracheal tube are retracted inferiorly; make sure tongue is not pinched by the teeth to avoid necrosis or excessive swelling.
- Soft palate and uvula retracted superiorly
- Use fluoroscopy or lateral radiography before draping to determine the extent of the exposure.
♦ Intraoperative
Exposure
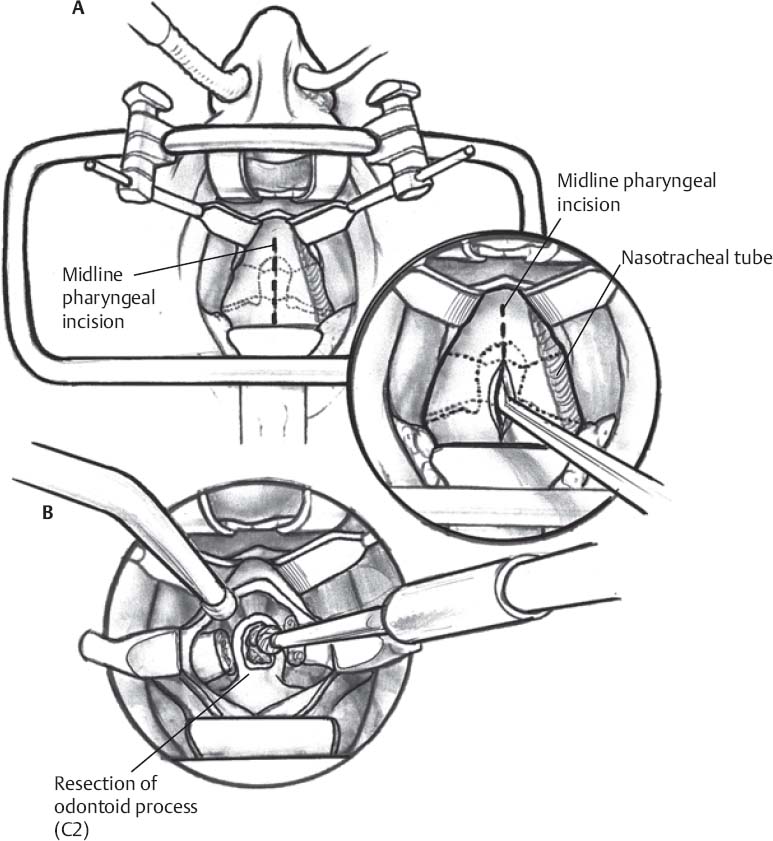
- Midline incision with either scalpel or Bovie through the posterior pharynx (Fig. 87.1A)
- Take down to bone in one layer and elevate subperiosteally; insert additional self retaining pharyngeal muscle retractors.
- With curettes and/or periosteal elevators, expose the clivus, anterior arch of C1, lateral margins of the odontoid, and body of C2.
- Remove the inferior portion of C1 arch to expose the base of the odontoid.
Odontoid Resection
- Divide the alar and apical ligaments from the tip of the odontoid with curved curettes.
- Transect the base of the odontoid process at the body of C2 with a high-speed drill and cutting bit to the posterior cortex.
- The posterior cortex can be removed with a small Kerrison or diamond drill bit with irrigation (Fig. 87.1B).
- Once the odontoid has been completely transected, it can be grabbed with a pituitary rongeur and pulled ventrally.
- Any remaining compressive soft tissue can be removed in a piecemeal fashion. The transverse ligament can be divided to expose the dura and confirm adequate decompression.
- Close pharyngeal muscles and remaining ligaments in one layer with interrupted 2–0 Vicryl suture.
- Pass a nasogastric feeding tube under direct microscopic vision to avoid damaging the incision.
♦ Postoperative
- Place patient in a hard cervical collar immediately after surgery.
- Leave intubated for 24 hours after surgery or until tongue swelling subsides. Observe in intensive care unit for 24 hours after extubation with an emergency airway cart in the room.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


