♦ Preoperative
Operative Planning
- Patient counseling regarding risk, benefits, and postoperative course
- Appropriate imaging
- Plain x-rays
- Determine number of ribs for localization
- Assess deformity and/or instability
- Determine number of ribs for localization
- Magnetic resonance imaging (MRI)
- Determine extent of neural element compression
- Computed tomography (CT)
- Evaluate bony anatomy
- CT/myelogram
- If MRI contraindicated
- Plain x-rays
Routine Equipment
- Basic spine tray including Kerrison rongeurs (2 to 4 mm)
- Cautery: monopolar and bipolar
- High-speed drill (e.g., Midas Rex)
- Headlight and loupe magnification
Special Equipment
- Cell saver: if significant blood loss anticipated in the absence of infection/neoplastic disease
- Microscope: for intradural pathology
Operating Room Set-up
- Prone table: Jackson table with Wilson frame or bolsters
- Mayfield head holder versus Gardner Wells tongs with traction
- Intraoperative anteroposterior and lateral x-ray versus fluoroscopy
- Secure endotracheal tube for prone position
- Appropriate blood pressure monitoring
- Foley catheter for extended cases (beyond 3 hours)
- Perioperative antibiotics 30 minutes prior to skin incision
- Perioperative steroids for decompressive or intradural pathology
- Avoid any orbital compression if patient’s face placed on cushioned mask
♦ Intraoperative
Positioning
- Prone position
- Arms tucked along side for pathology rostral to T6–T7
- Head secured with Mayfield head holder or Gardner Wells tongs and 15 lb of traction
- Arms placed on cushioned boards for pathology caudal to T6–T7
- Arms tucked along side for pathology rostral to T6–T7
- Maintain exposure of posterior iliac crest if fusion intended
- Ensure that patient is well secured to the operative table in case rotation of the table is desired to enhance ventral visualization.
Sterile Prep
- Shave with disposable razor
- Standard scrub and prep
Incision Localization
- Anteroposterior x-ray used to localize spinal level
- Requires preoperative verification of rib number
Exposure
- Midline incision
- Subperiosteal dissection of paraspinal muscles off spinous processes and lamina to the lateral extent of transverse process
- Verify level with intraoperative x-ray
- Placement of self retaining retractors (e.g., Weitlaner or Adson-Beckman)
- Clear intralaminar soft tissue with curettes/rongeurs
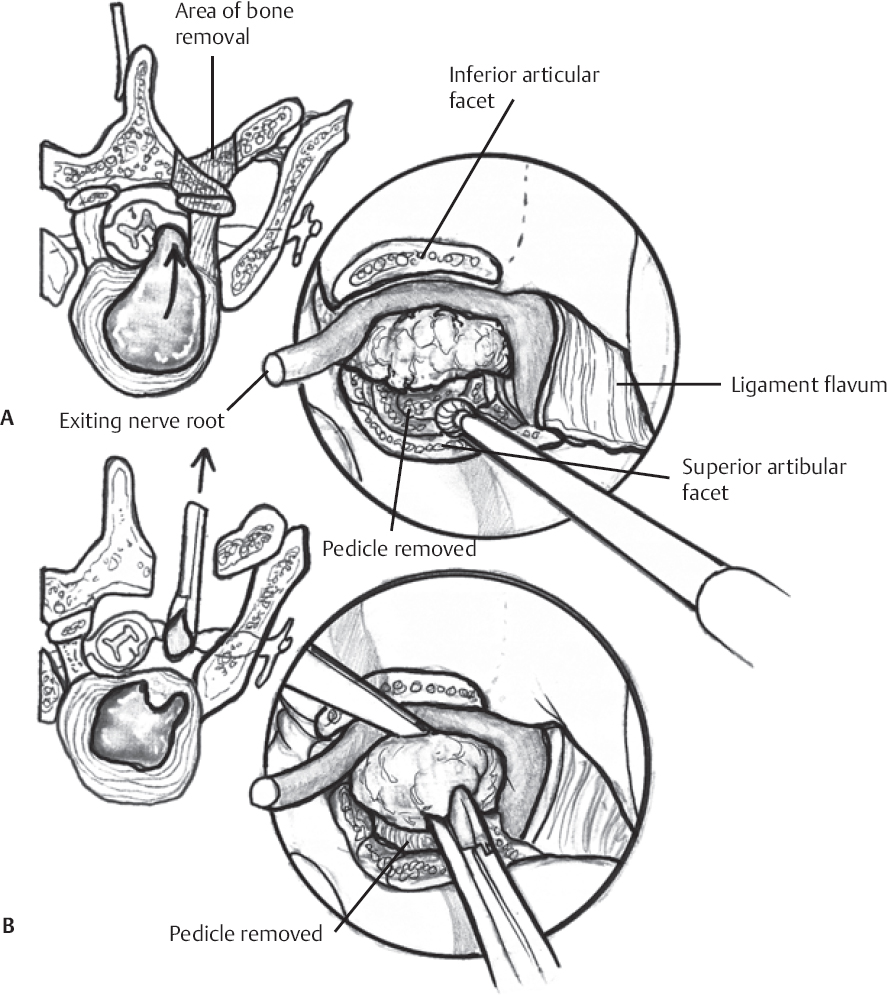
Bone Removal (Fig. 122.1A)
- Direct entry into the pedicle is achieved by carefully decorticating the junction of the pars and superior facet with a high-speed drill.
- The pedicle entry site is identified by the blush of cancellous bone.
- The pedicle can also be located through a laminectomy or laminotomy.
- The lateral aspect of the ligamentum flavum is resected to reveal the lateral surface of the thecal sac and exiting nerve root.
- Resection of the surrounding superior facet and pars with Kerrison rongeurs allows identification of the remaining cortical surfaces of the pedicle.
- The lateral aspect of the ligamentum flavum is resected to reveal the lateral surface of the thecal sac and exiting nerve root.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


