Chapter 66 Trauma Surgery
Thoracic and Thoracolumbar Junction
Approximately 160,000 patients a year in the United States suffer traumatic spinal column injuries, with 10% to 30% of them having a concurrent spinal cord injury.1–4 The majority of these injuries consist of cervical and lumbar (L3-5) spine fractures. However, between 15% and 20% of traumatic fractures occur at the thoracolumbar junction (T11-L2), whereas 9% to 16% occur in the thoracic spine (T1-10).5,6 Forces along the long stiff, kyphotic thoracic spine catalyze an abrupt switch into the mobile lordotic lumbar spine at the thoracolumbar junction. Biomechanically, this transition zone is susceptible to injury and is the most commonly injured portion of the spine. High-energy trauma (i.e., motor vehicle accidents) is the leading cause of injury over this region, followed by falls and sports-related injuries.7 Men are at four times higher risk than women. Because of the higher-energy mechanisms of injury, involvement of other organ systems is encountered in up to 50% of thoracolumbar trauma patients.7 These high-energy injuries, such as those causing thoracic-level paraplegia, have a first-year mortality rate of 7%.3,8
Anatomy
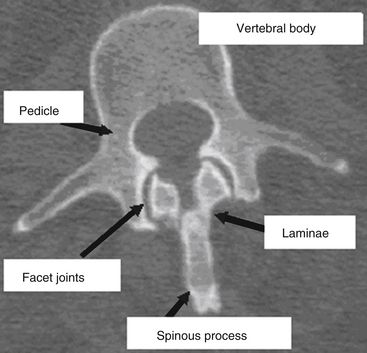
The vertebral column provides humans with the ability to maintain an upright posture, protects the neural and visceral organs (i.e., heart, lungs, abdominal contents), and helps with motility. It consists of 29 vertebrae arranged in 4 major curves, 2 primary curves (thoracic and sacral), and 2 compensatory or secondary curves (cervical and lumbar).9 The vertebral column also provides a protective environment for the spinal cord and neural elements. The vertebral body, pedicles, and dorsal elements surround the spinal cord, permitting the spinal nerves to exit through the paired neural foramina. The laminae are formed as dorsomedial extensions of the pedicles and fuse in the midline to create the spinous processes (Fig. 66-1). Nomenclature for the thoracic spine varies; however, in this chapter the thoracic spine is considered to span T1 through T10, and the thoracolumbar junction T11 through L2.
Primary spinal curves are present at birth, are maintained through life, and are relatively rigid or stiff. Secondary curves are more flexible and result from development or adaptation. The first secondary curve is the development of cervical lordosis at approximately 3 to 9 months of age as the infant begins supporting his or her head and sitting upright. The lumbar lordosis develops later (between 12 and 18 months), as the child begins to ambulate and assumes an upright posture.9 A thorough knowledge of the thoracic spine and thoracolumbar junction anatomy facilitates a greater understanding of the biomechanical, radiographic, and surgical techniques that are used to treat these fractures.
Thoracic Spine
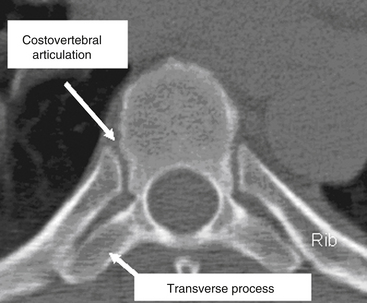
The thoracic spine differs from the cervical and lumbosacral spines as a result of its articulation with the rib cage (T1-12), extensive ligamentous support network, coronal facet joint orientation, and small spinal canal-to-neural element ratio (Fig. 66-2). The thoracic laminae increase in width and thickness from T1 to T12, and this prevents hyperextension.10 The anterior longitudinal ligament (ALL) provides further stability by increasing the tensile strength from T1 to T12. Moreover, the dorsal, ventral, and lateral diameters of the vertebral bodies increase from T2 to T12.11–15 The thoracic kyphotic curve results from the greater height of the dorsal vertebral wall as opposed to the ventral vertebral wall. The transverse pedicle diameters decrease from 9 mm at T1 to 5 mm at T5 and then increase in size distally to T12.14 In the sagittal plane, pedicle width increases from T1 to T11. However, in the transverse or axial plane, the thoracic vertebrae have a triangular configuration and appear heart shaped. There is significant variability in what is considered the “normal” sagittal curvature of the thoracic spine. This value has been reported to be between 20 and 45 degrees,13,16,17 with each individual vertebral body contributing approximately 3.8 to 3.9 degrees of kyphosis through its wedged-shaped angulation. This variability is further influenced by age (increases with age) and sex; women have a greater degree of kyphosis than men.16,17 There is also a significant degree of variability on a segmental basis, particularly at the transitional regions with the lordotic cervical and lumbar spines.12,18,19 The apex of thoracic kyphosis is typically located at the seventh thoracic vertebra, but varies with each individual. The thoracic spine typically has a mild, right-sided lateral curvature.9,17 The etiology of the right-sided lateral curve is debated but is believed to be either the result of hand dominance (right-hand majority) or created by pulsations of the thoracic aorta.9
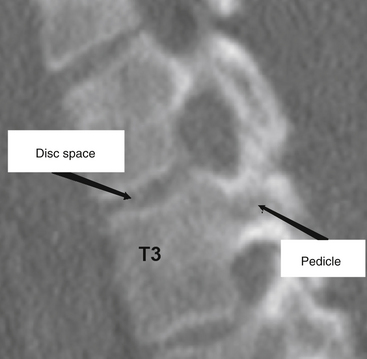
The thoracic pedicles are situated toward the rostral portion of the vertebral body, close to the superior disc space (Fig. 66-3). The pedicle angle decreases from T1 to T12; it is 251 degrees at T1 and 0 degrees at T12.11,17,20 The pedicle location on the vertebral body progressively migrates as the spine is descended in a caudal direction. The medial pedicle cortical wall is approximately two to three times thicker than the lateral wall.21
The thoracic transverse processes project laterally from the dorsal articular pillars and decrease in length caudally.5 However, unlike the lumbar spine, the relationship between the transverse process and the midpoint of the pedicle is not as clearly defined. McCormick22 showed that there is a significant degree of variability in the relationship of the transverse processes to the pedicles. The midpoint of the T1 transverse process is approximately 5 mm rostral to the center of the pedicle, whereas at T12 the transverse process-to-pedicle relationship changes to approximately 6 mm caudal.20 Comparatively, this transverse process to pedicle relationship is greater than 1 cm at both T1 and T2, and is approximately 0 cm when one analyzes T6 and T7.20
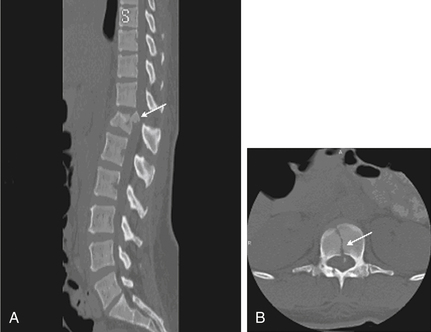
The thoracic spine facet articulations are considered apophyseal joints and are composed of a ligamentous capsule with a synovial lining. These ligaments in the thoracic spine are thicker than their cervical counterparts. In the thoracic spine, the costovertebral (rib-vertebra) facets are located anterior to the transverse processes. The isthmus of bone between each pair of superior and inferior facets is called the pars interarticularis, a site of fracture and bony nonunion for those with a condition known as spondylolysis. The joints are located at the rostral and caudal borders of the laminae and situated medial to the transverse processes (Fig. 66-4). The caudal facet’s ventral surface articulates with the rostral facet’s dorsal surface. Thoracic facet joints are oriented in a coronal plane and therefore limit the degree of flexion and extension of the thoracic spine.23
There are several key anatomic features that are essential for understanding the relationship of the ribs and the thoracic vertebrae. First, the ribs articulate with the thoracic vertebrae at two separate locations. The head of the rib articulates with the transverse process of the body at the costotransverse articulation, except at T1, T11, and T12. This articulation is supported with a large superior costotransverse ligament, which connects the rostral rib segment to the caudal transverse process (see Fig. 66-2). It also articulates with the disc space adjacent to the body above by virtue of the rib head of the same-numbered vertebral body articulating with it through the two costal hemifacets (T2-10).
The strong ligamentous structures that compose the costovertebral joint make the thoracic disc the strongest of all the vertebral discs.24 The superior hemifacet (rostral on the vertebral body and caudal to the rib) is located over the pedicle, such that the sixth rib articulates with the fifth and sixth thoracic vertebral bodies and overlies the sixth vertebral pedicle. Because of the rostral location of the thoracic pedicle on the vertebral body, the sixth rib overlies the T5 to T6 disc space. Understanding the anatomic relationship of the rib head with the pedicle allows the surgeon to remove the rib head and identify the neurovascular bundle, along with the neural foramina and thecal sac, at that level.
The spinal canal diameter varies throughout the vertebral column and is the narrowest in the midthoracic region (T3-9).11,13,25 The transverse spinal canal diameter decreases from T1 to T3 and then increases caudally into the lumbar region. The anteroposterior (AP) diameter, however, is more varied.13,25 Therefore, in the thoracic region a minor degree of canal encroachment can compromise the narrow canal and may result in neurologic compromise.26,27 Furthermore, the thoracic spinal cord has the most tenuous blood supply.13 Thus, small canal size, limited blood supply, and the high degree of energy required to create a thoracic fracture combine to result in a 90% incidence of neurologic deficit in patients who sustain a thoracic fracture.28
Thoracolumbar Junction
The transition from a relatively rigid thoracic kyphosis to a mobile lumbar spine occurs at the thoracolumbar junction. This transition generally occurs at T11 to T12, although in elderly female patients the thoracolumbar inflexion point migrates caudally as a result of their increased degree of thoracic kyphosis.12,17,19
The caudal thoracic ribs (T11 and T12) afford less stability at the thoracolumbar junction region compared with the rostral thoracic region because there is no connection to the sternum and thus they are “free floating.” Only a single rib articulation is present on the T11 and T12 vertebral bodies, and there are no accessory ligamentous attachments, such as the rib’s tubercle to the vertebral body by the costotransverse ligament, or the ligamentous attachment to the transverse process.9 The surrounding thoracolumbar ligaments, such as the interspinous and thoracolumbar fascia, are strongest caudally and provide a significant amount of stability.14
The thoracolumbar junction facet joints are again of the apophyseal type and are composed of a ligamentous capsule with a synovial lining. As mentioned previously, the joints of the midthoracic region are oriented in the coronal plane, limiting flexion and extension while providing substantial resistance to AP translation.5 In the lumbosacral region, the facet joints are oriented in a more sagittal alignment, which increases the degree of potential flexion and extension at the expense of limiting lateral bending and rotation. Depending on the spatial orientation of the spinal column (i.e., flexion or extension), the facet joints may support a third of the axial load. These joints, however, provide substantial support and resistance to approximately 35% to 45% of the torsional and shear forces experienced in this region.6,29
At birth, the spinal cord terminates at the end of the vertebral column or lumbosacral junction. However, the end of the spinal cord, or conus medullaris, migrates rostrally as the infant develops.30 In neonates the spinal cord terminates between the first and third lumbar vertebrae, whereas in adults it is positioned between the twelfth thoracic vertebra and the second lumbar vertebra.30
Imaging
It is not uncommon in clinically unstable trauma patients for fractures not to be identified early in the resuscitative period. It has been reported that between 5% and 15% of multisystem trauma patients have occult fractures not diagnosed on their initial evaluation.31–33 Although thoracic vertebral fractures make up only a minor proportion of traumatic fractures, they are extremely difficult to visualize compared with other vertebral or appendicular fractures. Approximately 20% to 50% of superior thoracic spine fractures are not diagnosed on admission plain radiographs.5,34,35 Therefore, all suspected spine trauma patients should be immobilized on admission until a thorough and detailed spinal evaluation can be performed. If appropriate stabilization precautions are not taken in this patient population, unforeseen neurologic compromise may result.6
Initial radiographic assessment includes AP and lateral spine films. The AP film should be examined for loss of vertical body height, fracture of the oval-shaped pedicles, increased interpedicular distance, transverse process or rib fractures, and malalignment of vertebral bodies or spinous processes without a history of scoliosis. The lateral radiograph should be examined for loss of body height, disruption of the rostral or caudal end plate, dorsal cortical wall fracture with retropulsed bone, fracture of spinous processes, widening of interspinous distance, and subluxation or angulation of vertebral bodies.36 Malalignment in any plane, but especially in the AP plane, suggests the possibility of a fracture-dislocation.12 Plain radiographs may not be accurate in determining the involvement of the posterior vertebral wall with a thoracic fracture.37,38
Plain radiographs are particularly useful in assessing the patient’s overall sagittal and coronal balance. If a deformity exists, a useful radiographic technique to determine the degree of deformity is measurement of the Cobb angle, which is the subtended angle measured between a perpendicular line drawn from the superior end plate of the vertebral body above the injured vertebral body and the inferior end plate one level below the injured body (see Fig. 66-20). This method of measuring spinal sagittal angulation has been shown to have the highest degree of intraobserver and interobserver reliability.39
In the presence of a vertebral body injury, the entire spine should be imaged in an orthogonal manner because of the high incidence (5–20%) of noncontiguous spine fractures.40–42 The rostral thoracic spine can be difficult to visualize on lateral plain radiographs because of the patient’s shoulders and body habitus, and a swimmer’s view may provide better visualization of the cervicothoracic junction down to the T3 vertebral body.43 Radiographically, a typical superior end-plate thoracic fracture shows loss of vertebral height, with or without malalignment, a widened paraspinal line, and possibly a widened mediastinum.35 Because of difficulties in imaging the upper thoracic region (T1-4), a high index of suspicion is required on the physician’s part to avoid missing injuries at this level. The physician should have a low threshold for ordering supplemental imaging modalities to assist in the diagnosis, such as CT and MRI.
Computed Tomography
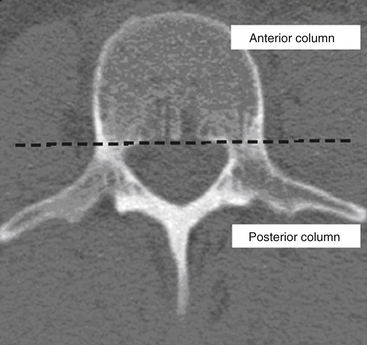
CT is more sensitive in detecting fractures than plain radiographs44 (see Fig. 66-4). It can also define the three-dimensional anatomy of complex fractures through reformatting in the sagittal and coronal planes. CT better delineates the bony structures once an injury is identified.45–47 CT reveals the integrity of the middle column and the degree of canal compromise, as well as subluxations or fractures of facets and laminae. The presence of two vertebral bodies on the same axial cut of a CT scan may indicate a fracture-dislocation, but first the radiographer must ensure that the gantry has been angled parallel to the vertebral end plates. Sagittal reconstructions are helpful in visualizing flexion-distraction injuries and fracture-dislocations. Serial CT scans of lumbar fractures have confirmed spontaneous remodeling and the reabsorption of retropulsed bone fragments in the spinal canal at long-term follow-up.48–50
CT image reconstruction is also invaluable at the cervicothoracic junction because of the overlap of the scapula, shoulders, and surrounding tissues. In the obtunded patient, this technique has been reported to identify more than 10% of fractures not visualized on plain radiographs.51 CT, however, has a limited capacity to visualize disc herniations, epidural or subdural hematomas, ligamentous disruption, and spinal cord parenchymal changes.52
Magnetic Resonance Imaging
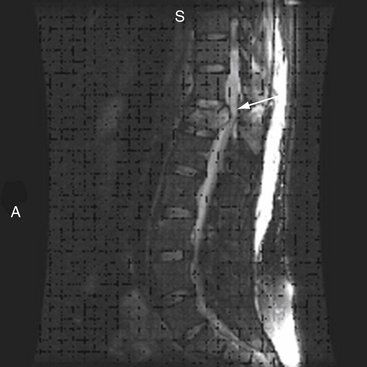
MRI has further improved the ability to visualize and comprehend the pathoanatomy of soft tissues, ligaments, and intervertebral discs, and the neural element disruption that occurs after spine injury. Unfortunately, MRI is not always available because of its expense, because it takes longer to implement, and because it cannot be performed on patients with ferromagnetic implants. Today it has supplanted CT myelography as the imaging tool of choice for the neuraxis because it is faster and noninvasive and allows improved visualization of the spinal cord parenchyma.53 MRI provides the physician with the ability to identify edema and/or hemorrhage of the spinal cord53 (Fig. 66-5). These images have been correlated with neurologic outcomes, where the presence of hemorrhage in the spinal cord parenchyma is associated with minimal neurologic recovery.54

MRI evaluation is especially useful at the thoracolumbar junction because of the variable location of the cauda equina and conus medullaris in the adult population at this level.55 A neurologic examination can be difficult to interpret at the conus-cauda equina transition level as a result of the presence of lumbar spinal nerve sparing, the presence of concurrent injuries, sedation, or indwelling catheters, and delayed reflex recovery (Fig. 66-6). Accurate neural visualization may help in clarifying the pathoanatomy in these clinical situations.
Biomechanics
The vertebral body is the primary load-bearing structure of the spine, with the intervertebral disc transferring all forces applied to the adjacent vertebral bodies.56,57 The anulus fibrosus of the intervertebral disc supports a significant portion of all applied axial and lateral loads and resists tension and shearing.58
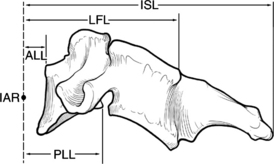
The spinal ligamentous structures are essential in maintaining overall sagittal balance. The posterior longitudinal ligament (PLL) is a relatively weak ligament that provides some restriction to hyperflexion, along with the ligamentum flavum. The thicker ALL functions in resisting spinal hyperextension and distraction.59 This thick ligament has fatigue loading values that are approximately double those of any other spinal ligaments,57–59 and its strength increases caudally from C3 to the sacrum.59 The intrinsic strength of the spinal ligaments is only an isolated factor in the overall stability of the spinal column. The lever arm by which these ligaments act on the spine also significantly affects the overall stability of the vertebral column (Fig. 66-7).
Abnormal motion patterns and coupling can be an indication of clinical instability, which ultimately must be treated in some manner. Clinical instability can be quantitatively measured in respect to the moving segment’s instantaneous axis of rotation (IAR). The IAR is an axis about which a vertebra rotates at some instant of time.46 This axis is a geometric concept and does not apply to a specific anatomic location.60 However, in the normal thoracic and thoracolumbar spine, the IAR is located in the ventral vertebral body. For normal spinal units, the IAR for each of the rotary modes (flexion, extension, lateral bending, and axial torsion) is confined to a relatively small area somewhere within the spinal unit.14 The facet capsules are very strong ligaments and act with a short lever arm by their relationship to the IAR, whereas the intraspinous ligaments are relatively weak but act with a great lever arm because of their increased distance from the IAR. Based on the ligaments’ relative strengths, it would seem that the intraspinous ligaments are not important, but both ligaments significantly affect the strength and structure of the spine.
The thoracic spine differs from the remainder of the spinal column because it is supported by and maintains articulations with the ribs (see Fig. 66-2). The intact rib cage increases the axial load-resisting capacity of the thoracic spine by a magnitude of four. The rib cage and facet articulations limit rotation, and therefore most thoracic spine fractures occur from a flexion or axial compression force vector.61 The majority of stability in flexion is provided by the costovertebral articulations.62 A significant factor in the degree and extent of fracture character is the rate of force impact loading.63
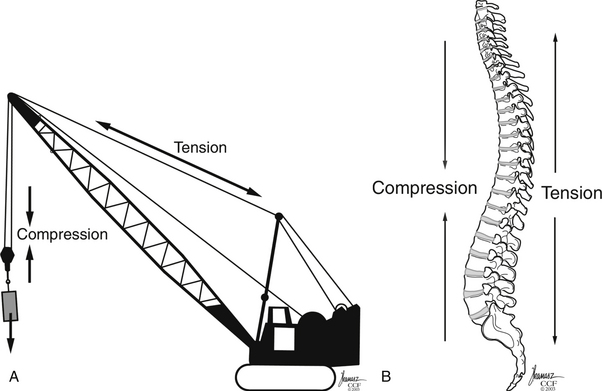
Gravitational forces exert a significant axial load on the vertebral column in the standing adult human. The center of gravity of the body, located where all forces are counterbalanced such that there is no net movement, is approximately 4 cm anterior to the first sacral vertebra.14 This results in a ventral bending (angular) vector acting on the spinal column. This bending force draws or attracts the ventral spinal column closer to the center of gravity such that a lower energy state may be achieved by the paraspinous musculature. The dorsal ligamentous complex and dorsal paraspinal musculature, acting as a tension band, counteracts these forces, such that the net sum of the vectors acting on the spine equals zero. Therefore the dorsal ligamentous, osseous, and muscular components are essential for overall support of the spine to prevent a change in the spine’s sagittal alignment. Trauma resulting in disruption of the spinal ligaments or osseous structures may change the net vector sum from zero, resulting in the potential for spinal imbalance. These new vectors acting on the spine, if not corrected, may result in a gradual spinal deformity with or without associated pain or neurologic deterioration. Whiteside used the analogy of a construction crane to illustrate this mechanical principle64 (Fig. 66-8). In this analogy, the weight to be lifted is ventral to the crane, where the boom (anterior vertebral column) is under compression and the guidewires (posterior columns) are under tension. Failure of either supporting structure independent of the other will result in mechanical failure or collapse.
The thoracic and thoracolumbar vertebrae are at increased risk for development of compression fractures after trauma as a consequence of axial loads resulting from the natural kyphotic curvature of the thoracic spine.65 The kyphotic posture results in the placement of axial forces on the ventral portion of the vertebral body. An axial load causes all points that are ventral to the IAR of the spine to come closer together while simultaneously all points that are dorsal are spread apart. Therefore, if the strength of the ventral vertebral body is exceeded, a fracture of the vertebral body occurs, resulting in a vertebral compression fracture (VCF). The traumatic forces may also exceed the strength of the dorsal vertebral body and ligamentous elements, resulting in disruption of the dorsal tension band. The destruction of the ventral vertebral stabilizing elements (i.e., vertebral body, disc, ligaments, anulus) causes the IAR to migrate dorsally to the region with intact supporting structures.65,66 Dorsal migration of the IAR causes the previous mechanical advantage of a longer level arm from which the dorsal ligaments and muscles acted to be shortened. This migration of the IAR also simultaneously increases the distance of the center of gravity to the IAR, thereby placing further distraction on the dorsal spinal column and compression on the ventral spinal column65,66 (see Fig. 66-7).
Concurrent Injuries
Thoracic Spine Fractures
The thoracic spine’s structural integrity—the interaction of its osseous structures and ligaments and the rib cage—provides more protection against potential fracture than the remaining vertebral column. Hence, when a fracture occurs over this region, the physician must be aware that a high degree of energy was required to produce this lesion. These forces on impact are transmitted to the soft tissue and viscous elements contained within and around the thoracic cavity, resulting in a high incidence of concurrent injuries. The incidence of concurrent injuries is reported to be greater than 80%, involving the thorax, appendicular skeleton, and abdominal region.35,42,67 These high-energy impacts also affect areas remote from the trauma, such as the cranial vault. Petitjean et al.67 reported a 65% incidence of head injuries after high-velocity impacts that resulted in incomplete thoracic spinal cord injury, with 12% of these injuries classified as severe (Glasgow Coma Scale score <8).
Tearing or rupture of the aorta has been associated with thoracic vertebral fractures.68 Hemodynamic instability may result from injury to any vascular structure, or even from blood loss secondary to a thoracic vertebral fracture.67,69,70 Hemothorax has also been reported to occur in 24% to 32% of patients with thoracic fractures.71,72 Pulmonary injuries have been reported in 85% of patients and typically consist of pulmonary contusions.28 Infrequently, perforation of the esophagus and tracheal injuries have also been associated with thoracic fractures.73–75 The mechanism of perforation is believed to be ischemia of the esophageal tissue after becoming devascularized as a result of a deceleration-traction injury.73,75
Thoracolumbar Junction Fractures
The thoracolumbar region is more vulnerable to concurrent injuries than the thoracic region because it is not provided the protection of the thoracic rib cage. Petitjean et al.67 reported a 71% incidence of associated blunt abdominal injuries after thoracolumbar fractures. Typically, these consist of hollow viscus injuries (e.g., intestinal perforation), mesenteric avulsions, or solid organ injuries.28,67,76
The most common mechanism of abdominal injury is the distraction or seat belt injury.28,67,77 Blunt abdominal aortic dissections are associated with distraction-rotation injuries of the thoracolumbar region.2,77 These aortic injuries can range from an intimal tear to a full-thickness laceration. CT provides accurate imaging of this injury in the stable and asymptomatic patient. A large degree of energy is involved in this distraction-type mechanism, accounting for the large number of associated injuries. Multiple-level thoracic and lumbar fractures are also associated with a high incidence of abdominal injuries.2
Axial load injuries, particularly in patients who have jumped or fallen and landed on their feet, may manifest as both thoracolumbar fractures and calcaneal fractures. Isolated transverse process fractures of the lumbar spine should not be overlooked as a minor injury. Miller et al.78 reported a 48% incidence of concurrent abdominal injuries associated with transverse process fractures. Therefore, a physician treating vertebral column injuries must be aware not only of the presence of spine fractures but also of the possibility of concurrent, nonspinal, soft tissue and bony injuries.
Classification
Injuries to the thoracic and lumbar spine account for more than 50% of all spine fractures and a large portion of acute spinal cord injuries.17 Given this frequency and the significant impact of these injuries, significant advances have been made in the surgical treatment of thoracolumbar trauma. Nevertheless, although there has been progress in the invention and evolution of spinal instrumentation and surgical techniques, medical decision making in spine trauma remains controversial. To this day, fracture treatment can vary widely, from bracing to invasive 360-degree fusions, based on geographic, institutional, or individual preferences with little scientific basis.
A number of classification systems have been developed in an attempt to better define thoracolumbar trauma and aid treatment decision making. These systems are typically based on either anatomic structures (Denis three-column system) or on proposed mechanisms of injury (Ferguson and Allen).79,80
In 1931 Watson-Jones pioneered one of the first spinal fracture grouping systems by type.81 This schematic categorization was based on diagnostic and treatment of flexion injuries.82 This was followed by Nicholl,83 who developed the first detailed thoracic and thoracolumbar spine fracture classification scheme and attempted to define unstable versus stable fractures after trauma in a series of flexion and flexion-rotation injuries. This classification system was originally intended to guide the treatment and work status of injured miners. Nicholl emphasized the importance of the dorsal interspinous ligament in spinal stability.83 Later, Holdsworth,84 after clinical failures in immobilizing pure flexion fractures following the recommendations of Watson-Jones, further studied the importance of the spinal ligamentous complexes after thoracolumbar junction injuries. He classified fractures, according to their mechanism of injury, into four main types: flexion, flexion and rotation, extension, and compression. Holdsworth84 further classified these fractures as unstable if the posterior ligamentous complex, consisting of the intervertebral disc, spinous ligaments, facet capsules, and ligamentum flavum, was disrupted. He noted that in compression, flexion, and extension injuries, the dorsal ligamentous complex is typically not ruptured and these fractures were therefore considered stable. However, he reported that flexion and rotational injuries were at a much greater risk for disruption of the dorsal ligamentous complex and subsequent instability. Subsequently, Rennie and Mitchell85 added a fifth category of thoracolumbar junction fractures consisting of flexion-distraction fractures or seat belt injuries, based on the description and reporting of Chance.86
Kelly and Whiteside87 reported that without dislocation of the dorsal elements of the spinal column, neurologic injuries rarely occur. They classified fractures based on structural criteria and considered the spine to consist of not one, but two separate supportive columns (Fig. 66-9). The primary weight-bearing ventral column is composed of the vertebral bodies, and a second structural column consists of the posterior neural arches and ligaments. The structural classification scheme provided surgeons the ability to predict the degree of instability of the spine based on the degree of resulting structural damage after trauma. Based on this assessment, treatments were devised to enhance neurologic and spinal stability. Later, Louis88 modified this structural classification scheme by proposing a third column. Louis’s three-column concept consisted of one ventral column, the vertebral bodies, and two dorsal columns involving each facet articulation (Fig. 66-10).
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


