Low-grade isthmic spondylolisthesis in adults occurs in approximately 5% of the population and is frequently a relatively benign disease entity. The degree of anterior slippage in isthmic spondylolisthesis can be rated using four grades, according to Meyerding (
1), but the relation between the degree of listhesis and the level of complaints such as low back pain and sciatica remains somewhat unclear. For example, in a considerable number of asymptomatic patients, the spondylolytic defect and associated slip are discovered during routine x-rays taken for other reasons. This is one of the reasons why specific treatment for isthmic spondylolisthesis is still not completely clarified.
WHAT ARE THE THERAPEUTIC OPTIONS?
Some patients can benefit from conservative treatment including physical therapy, braces, or pain medication. With regard to surgical treatment there are several different options, of which posterolateral fusion with instrumentation is generally considered to be the gold standard of treatment.
Table 25.1 lists some of the most common procedures with some of the positive and negative aspects of each treatment, respectively.
Because of the many controversies regarding the optimal treatment strategy, a systematic review of the literature was performed, which is reported in this chapter. The aim of the study was to determine which surgical technique provides the best clinical and radiologic outcome in adult patients with low-grade lumbar isthmic spondylolisthesis. A secondary aim was to find out for each of the fusion techniques described what the clinical and radiologic results were, what degree of reduction of the spondylolisthesis was achieved with the procedure and what loss of this correction occurred postoperatively. Of further interest were the lordotic angles before and after the surgical procedure, adjacent segment degeneration, as well as associated complications.
METHODS
To obtain all the relevant literature, we used a sensitive search in the most common databases of published literature: the Cochrane Database of randomized controlled trials (2004 issue 1), Current Contents (1996 to March 2004), Medline (through PubMed; 1966 to March 2004), and Embase (through March 2004).
The search strategy was adopted for the different databases. We made no restrictions on language or date. From the articles that were selected, the references were screened for further articles.
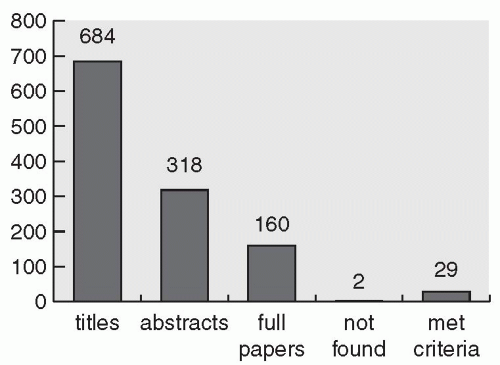
All articles were selected by two independent reviewers. The selection was not blind but during selection of the titles and abstracts, the rest of the information was masked. The articles were selected on basis of title and abstract with the following criteria:
The intervention(s) used had to include at least one surgical intervention. Type of instrumentation used, the performance of a decompression, and the possible intention to reduce the listhesis had to be stated in the article. Some studies did not mention all of these minimal criteria. These studies were included but were used as a separate group in the best evidence synthesis.
The indication for surgery had to be adult low-grade (Grade 1 and 2, or <50%) isthmic spondylolisthesis at one lumbar level that did not respond to conservative treatment. The study population had to include a minimum number of 10 patients. When the isthmic spondylolisthesis group was a subgroup (<95%) of a study population, results for this subgroup had to be given.
Outcome parameters had to be a radiologic, clinical, or functional measure. For example, the 36-item Short-Form Health Survey (SF-36), Western Ontario MacMaster (WOMAC), or Oswestry Disability Index (ODI) questionnaires; pain scores; accomplished fusion rates; and complications. The selected articles had to be published in peer-reviewed journals.
METHODOLOGIC QUALITY OF INCLUDED STUDIES
According to the van Tulder criteria, only 4 of the 8 randomized trials were rated as a “high quality” study. High quality according to the Cowley criteria was awarded to only two of the five noncontrolled studies.
 Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage
Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage
 Mechanics of Neurological Impingement
Mechanics of Neurological Impingement
 Children
Children
 Surgical Treatment of High-Grade Spondylolisthesis: An Analysis of 18 Patients
Surgical Treatment of High-Grade Spondylolisthesis: An Analysis of 18 Patients
 Video-Assisted ALIF with Cage and Anterior Plate Fixation for L5-S1 Spondylolisthesis
Video-Assisted ALIF with Cage and Anterior Plate Fixation for L5-S1 Spondylolisthesis
 Bone Graft Alternatives in Spinal Surgery
Bone Graft Alternatives in Spinal Surgery



