Treatment of Lumbar Spondylolisthesis and Related Unstable Spinal Lesions: The Usefulness of PLIF with Cages and Semirigid Interpedicular Posterior Fixation for Circumferential Arthrodesis and Prevention of Adjacent Degeneration
Gilles Perrin
Posterior lumbar interbody fusion (PLIF) with cages is optimal not only for intervertebral fusion but also in re-establishing weight bearing to the anterior structures and in restoring the disc height and foraminal opening for nerve root decompression (1,2,3,4). Posterior fixation is indicated for immediate stabilization in order to enhance osteogenesis and to allow early mobilization without external contention in order to prevent muscle atrophy and spinal balance deterioration. PLIF as a distractive technique and posterior interpedicular fixation in compression restore physiologic lordosis and indeed protect the adjacent spine. Semirigid fixation with an interpedicular damper significantly reduces the risk of screw fracture and enhances the bone fusion by maintaining constraints on the cages. Prevention of adjacent degenerative disease by using semirigid extension to the overlying vertebra of the posterior interpedicular fixation as a nonfusion method is indicated for protection of the adjacent spinal level in case preoperative imaging shows a pathologic disc adjacent to the forecasted fusion.
Delayed complications after lumbar fusion with recurrence of back pain and neurologic symptoms are now commonly reported and related to degenerative lesions at the adjacent intervertebral level above a fused spinal segment (5,6,7,8). A retrospective study reported by Gillet (9) on the fate of the adjacent motion segment pointed out that 41% of the patients with follow-up over 5 years developed transitional segment alterations such as collapsed discs, osteophyte formation with degenerative spondylolisthesis, or stenosis, and 20% needed a second surgery for extension of the fusion. This adjacent degeneration is related to reactional hypermobility and biomechanical hypersolicitation above a rigid fused segment (10,11,12). The reported rate of symptomatic adjacent segment disease in a meta-analysis of the literature performed by Park et al. (13) is higher in patients with transpedicular instrumentation (12.2% to 18.5%) than in patients who underwent fusion with other forms of instrumentation or with no instrumentation (5.2% to 5.6%). Logically, the risk of such adverse effects of fusion is related to the length of the fusion and the presence of preoperative degenerative discal lesions above the forecasted fusion (14,15). If monosegmental fusion is with very low adjacent reactional hypersolicitation,
bisegmental fixation indicated by severely slipped spondylolisthesis requires protection of the adjacent disk through the creation of a transitional zone between the fused vertebral segments and the overlying hypermobile spine (16). This intermediate zone can be protected by using a semirigid interpedicular element as a nonfusion method that allows controlled intervertebral motion (4 mm in flexion extension and 2 mm in vertical extension and compression).
bisegmental fixation indicated by severely slipped spondylolisthesis requires protection of the adjacent disk through the creation of a transitional zone between the fused vertebral segments and the overlying hypermobile spine (16). This intermediate zone can be protected by using a semirigid interpedicular element as a nonfusion method that allows controlled intervertebral motion (4 mm in flexion extension and 2 mm in vertical extension and compression).
The aims of this retrospective study were not only to assess the clinical outcome and fusion rate in the group of patients treated with circumferential arthrodesis achieved in one stage with a posterior approach, but also to determine in a subgroup of patients with long-term follow-up over 8 years the clinical and anatomical benefits of protection of the adjacent level by means of posterior semirigid stabilization in order to prevent recurrent symptoms.
MATERIALS AND METHODS
Study Design
From 1978 to September 2003, PLIF was performed in a personal consecutive series of 1,500 patients with clinical presentation of nerve root compression related to unstable bone or discoligamentous lumbar lesions such as
Isthmic spondylolisthesis, 1,095 cases (73%)
Foraminal stenosis with collapsed disc and degenerative spondylolisthesis, 259 cases (17.2%)
Lesions, documented by dynamic x-rays, which are either discoligamentous degenerative or iatrogenic unstable, 148 cases (9.8%)
In this series, 430 patients were operated on between 1993 and 2000 for lumbar stabilization of isthmic spondylolisthesis with circumferential arthrodesis in one stage through a posterior approach by using cages for PLIF and posterior interpedicular fixation and 290 patients were reviewed for clinical and radiologic evaluation with long-term follow-up (>4 years). Thirty-four of the 290 patients underwent surgery for isthmic spondylolisthesis between June 1993 and April 1997 with PLIF and posterior fixation and semirigid protection of the pathologic adjacent disc and were reviewed with a mean follow-up of 8.27 years to assess the evolution of adjacent spinal levels.
Surgical Procedure
The intervertebral space was approached posteriorly. The mobile posterior vertebral arch is completely removed. The lateral recesses and the foramina were widely open with total resection of the articular facets. Restoration of the intervertebral height in order to open the foramina and to achieve a total nerve root decompression was achieved by using distracting probes after discal resection. Such distraction with restoration of normal intervertebral discal height results in partial reduction of horizontal slippage. This partial reduction is sufficient for nerve root decompression. Total reduction of Grade 3 or 4 spondylolisthesis is not advisable because such reduction creates reactional excessive constraint to the overlying spine with a high risk of adjacent degeneration. It seems more logical to preserve the acquired adequate sagittal balance between the spine and the pelvic incidence (17). Cortical bone of the vertebral endplates was carefully kept intact. PLIF to distract the disc space was performed by using large intervertebral cages filled
with cancellous bone from laminectomy. Cylindric or threaded cages were implanted in 50 cases. Large parallelepiped titanium cages were used in 290 cases, and since 1997 PEEK polymer ADONIS cages have been inserted for PLIF in 90 patients.
with cancellous bone from laminectomy. Cylindric or threaded cages were implanted in 50 cases. Large parallelepiped titanium cages were used in 290 cases, and since 1997 PEEK polymer ADONIS cages have been inserted for PLIF in 90 patients.
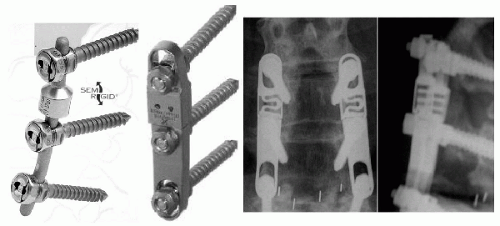 FIG. 19.1. Semirigid TTL rod and Aladyn plate-postoperative x-ray control of Aladyn plate.
Related posts: Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage Biomechanics of Spondylolysis with Reference to its Etiology, Diagnosis, Treatment, and Slippage
 Mechanics of Neurological Impingement Mechanics of Neurological Impingement
 Children Children
 Surgical Treatment of High-Grade Spondylolisthesis: An Analysis of 18 Patients Surgical Treatment of High-Grade Spondylolisthesis: An Analysis of 18 Patients
 Posterior Lumbar Interbody Fusion (PLIF) in Spondylolisthesis Posterior Lumbar Interbody Fusion (PLIF) in Spondylolisthesis
 Bone Graft Alternatives in Spinal Surgery Bone Graft Alternatives in Spinal Surgery
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|