2 Using Cerebral Vaso-Reactivity in the Selection of Candidates for EC-IC Bypass Surgery
Introduction
Since the failure of the EC-IC (extracranial-intracranial) bypass study in showing decreased risk of stroke after bypass,1 the utility of this procedure, particularly in chronic occlusive vascular disease (OVD), has come into serious question. Despite that failure in an unselected group of patients, anecdotal and clinical experience has lead clinicians who treat patients with occlusive vascular disease to conclude that there must be a subgroup of patients who are at a much higher risk of stroke than the general population who would still benefit from this procedure. This has lead to a great deal of research into the underlying pathophysiology in OVD and subsequently the development of a number of physiology-based techniques that are able to predict patients at increased risk of stroke. Once a technique has been established to identify a high-risk group, it then remains to be proven to decrease subsequent stroke risk when used as a selection tool for bypass. In order to understand the rationale for using cerebral vaso-reactivity (CVR) studies as a rational tool for the selection of candidates for flow augmentation surgery, a review of the pathophysiology is first necessary.
Physiology of occlusive vascular disease
Central to the physiology in carotid occlusion is the concept of cerebral autoregulation and its interrelationship with chemoregulation. Cerebral autoregulation is an intrinsic property of the cerebral vasculature that allows for maintaining consistency of CBF (cerebral blood flow) over a wide range of cerebral perfusion pressures (CPPs). This property is not unique to the cerebral vasculature, and involves very tight molecular regulation, allowing very precise, second-to-second adaptation to changing stresses. It is important to emphasize that this is an intrinsic property of the vessels, and is separate from other chemical or neural mediators of CBF adaptation. The molecular mechanisms are signaled by stretch of the vasculature, which initiates a phospholipase C mediated cascade, resulting in inhibition of calcium-activated potassium channels in smooth muscle, leading to smooth muscle contraction. The opposing forces are likely related to the cellular metabolic activity within neural and glial cells leading to activation of the same potassium channels and vasodilatation.2
An alternate method of testing the state of autoregulation involves testing vascular reactivity. This approach involves performing a baseline study to assess CBF, followed by a vasodilatory challenge and repeat of the study. The challenge can be as simple as breath holding to increase pCO2 or inhalation of CO2 gas—both relying on the principle that increasing brain CO2 acidifies the tissue and leads to vasodilatation (called chemoregulation). Alternatively, a cerebral vasodilatory agent such as acetazolamide that blocks carbonic anhydrase can be administered to induce tissue acidification and vasodilatation. These methods do not alter the underlying state of intrinsic autoregulation or metabolism, but they are able to determine to what degree the vessels can respond to such a challenge. In normal brain vasculature, a vasodilatory agent should lead to an increase in CBF by a certain percentage over the baseline level (typically 15% to 40%). If the vasodilatory agent does not cause an increase in CBF, one can conclude that the vessels have reached a maximal level of autoregulatory vasodilatation. In some cases, one may even see in one or more vascular territories a paradoxical drop in CBF in response to a vasodilatory challenge. This has been referred to as a “steal” phenomenon, where the portion of the vasculature that has a normal blood supply dilates normally in response to the challenge while the vascular territory that is already maximally dilated, and most often dependent upon leptomeningeal collaterals, experiences a loss of collateral supply.3 This approach thereby identifies a vascular territory that has experienced a failure of autoregulation with a reduction of CBF and a state of maximal vasodilation, and potentially the tissue most at risk for infarction due to a progression of hemodynamic compromise.
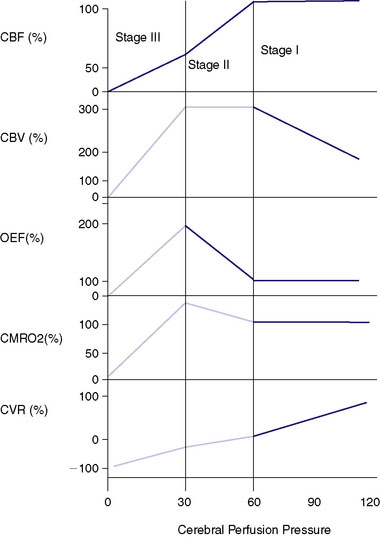
The cerebral vasculature has other adaptive mechanisms for compensating for decreasing perfusion pressure. Once the vessels are maximally dilated and the CPP continues to fall, the normally excessive levels of tissue nutrients (i.e., glucose and oxygen) carried within the blood supply begin to fall. A common measurement is the oxygen extraction fraction (OEF), which normally is less than 50% and rises with a progressive fall of CPP. With a fall of CBF below about 20cc/100 g/min, the oxygen reserves become exhausted and metabolism becomes compromised. The increase in OEF can be measured using positron emission tomography (PET), although there remains controversy regarding the most accurate method.4,5 This physiology underlies the now well accepted stages of hemodynamic insufficiency described by Powers et al.6,7 that with the progressive fall of CPP, CBF is maintained by vasodilatation with the rise of CBV. This is referred to as Stage I insufficiency. Stage II insufficiency involves the failure of autoregulation with a fall of CBF and a state of maximal vasodilatation and an increasing OEF. With a continued fall of CPP the brain enters Stage III, with progressive cellular death. This metabolic decline can be directly measured by the CMRO2 (cerebral metabolic rate of oxygen use) as a single PET study. A vasodilatory challenge study done in Stage III will show a loss of positive reactivity or a “steal” as described previously. Because OEF is a ratio of CBF and CMRO2, with progressive cellular injury the CMRO2 will fall and the OEF can potentially return to “normal” with an equally reduced CBF and CMRO2. This stage has been referred to as a progression of Stage III with “matched hypoperfusion”8-12,70 (Figure 2–1).
Techniques used for testing CVR
Xenon/CT
Xenon has been thought to be an ideal technique for CBF determination due to its ability to provide quantitative data safely. 133Xenon may utilize individual gamma counters or an array that integrates information. Regional or tomographic SPECT (single photon emission tomography) techniques are utilized to record the washout of Xenon from the brain tissue with end tidal values being utilized to obtain an assessment of arterial content. A vast amount of information about CBF has been gained with this approach that is, however, limited by the need for precautions with radioactive Xenon and the inability to resolve information below the surface of the brain. Xenon/CT offers the advantage of providing high-resolution CBF information with equal validity in the center as well as the surface of the brain. Stable Xenon, which is radiodense and similar to iodine, is also a noble gas, thus not requiring any concerns about environmental contamination. The technique involves the measurement of both the arterial concentration and tissue arrival of Xenon on CT, allowing for solving of the Kety-Schmidt equation by integral math for each of the ∼24,000 CT pixels. The validity of the technique has been confirmed by cross-correlation with destructive (microspheres,13 iodoantipyrine14), and in vivo (133Xenon,15 PET,16 thermal dilution flow probes17) CBF technologies. No permanent morbidity or death has been reported despite its wide use for over 25 years, and Xenon gas is generally considered safe.18
Xenon techniques including 133Xenon SPECT and Xenon/CT have been used for examining CBF in carotid occlusion even before the failure of the EC-IC bypass trial.19 It was clearly recognized, even at that time, that physiological methods must have some role in selecting these patients. One observational study noted that only a small minority of patients (two of 20) showed increased CBF after bypass compared to the test done before bypass.20 Initially, decreased baseline CBF alone was used to select potential candidates for bypass and of 25 patients with normal baseline CBF, no early strokes were seen with no bypass, while bypass was shown to normalize decreased CBF levels in seven of eight patients. At the same time, other clinicians, mainly in Scandinavia, began to explore the concept of testing the CVR by administration of acetazolamide, as described previously, in selecting patients using regional 133Xenon who might benefit from bypass.21
The failure of the EC-IC bypass trial, however, meant that the financial and practical ability to perform bypass surgery for OVD was relegated to a primarily research role. As the group in St. Louis began a natural history study to define the stroke risk associated with increased OEF,22 similar work was being done with regard to CVR. Rogg23 first demonstrated that patients with symptomatic carotid occlusion or stenosis can have very different patterns of response to acetazolamide challenge. Forty-five percent of patients showed normal baseline CBF that augmented with acetazolamide ipsilateral to the occlusion. Thirty-one percent started with low baseline flow, but still augmented appropriately with acetazolamide, while 24% showed either no response or decreased response to acetazolamide, regardless of baseline CBF. Later, the same Pittsburg group, in a prospective trial, showed that patients with symptomatic carotid stenosis or occlusion can be divided more specifically to better predict subsequent stroke. Patients with normal baseline CBF and normal CVR had a stroke risk of 4.4% (2/46) in the mean 24-month follow-up period compared to 36% (8/22) patients with baseline CBF < 45 cc/100 g/min in any territory on the affected side as well as CVR showing negative reactivity (steal) of >5%. This translated to a 12.6 times increased risk of stroke in the group with a severe compromise of CVR. Furthermore, the two strokes in the normal reactivity group were contralateral to the affected carotid side, and were both in patients with carotid stenosis rather than occlusion.24 This represented some of the first data clearly linking the importance of poor CVR to subsequent stroke. Further data from this group confirmed this association further, especially in carotid occlusion, where the stroke rate in the 19.6-month mean follow-up period was 10% (2/26) in patients with normal CVR compared to 26% (10/38) in the patients with steal.25
This data has been cross-validated in other institutions as well, where the stroke rate was found to be 0.5% to 2.4% annually with normal CVR (measured by 133Xenon SPECT) compared to a 21.8% annual stroke rate if CVR was impaired in patients with carotid or MCA (middle cerebral artery) occlusion.26 Another group from Japan found a 6% (3/47) stroke rate in patients with normal CVR compared to 35% (8/23) with poor CVR. Decreased CVR was also found to be the only factor that the group measured that was associated with an increased stroke rate.27 There are some limitations in all of these data, particularly with regard to sampling error. None of these are long-term prospective observational studies, and the inclusion varies in terms of methodology, specific definition of impaired CVR, stenosis versus occlusion, intracranial versus extracranial disease, and clinical status of the patient. That said, there seems to be very convincing evidence from several sources that in patients with OVD there is a dramatic, statistically significant increase in risk of stroke predicted by impaired CVR.
Despite the fact that there is no randomized, controlled data to support the use of CVR, there has been nonrandomized data accruing over many years. As mentioned, the use of CVR in assessing patients with OVD began in the mid-1980s concurrent with the publication of the bypass trial. Vorstrup21 showed some of the first physiological data supporting the use of CVR in bypass selection. Adequate reactivity was defined as at least 13% flow augmentation from normal control data. Eighteen patients were bypassed for clinical reasons, nine of whom showed decreased CVR on acetazolamide testing, two of whom showed negative reactivity. Postoperatively, all of these patients showed improved CVR, but the two with negative reactivity were the only two whose baseline CBF increased. None of the remaining nine patients who were bypassed with normal CVR showed increased CBF postop, likely suggesting the lack of hemodynamic stress. The authors concluded that a randomized controlled trial was needed to assess this technique.21 Groups in Japan have also been using the technique in evaluating patients for bypass. In one study, 15 patients were studied before and after bypass. Three showed decreased CVR (again defined by normal controls), which improved after bypass. Furthermore, six patients had decreased baseline CBF and CVR pre-operatively. In three of these, the baseline CBF improved, and in four, the CVR improved postop.28 These early studies showed that in patients with impaired CVR, bypass can improve these physiologic parameters.
The next important step is to link whether bypass can decrease stroke risk in selected patients, and there have been some preliminary studies addressing this question. Kuroda29 first used CVR as a selection criterion for bypass in patients with OVD. Out of 32 patients, six who showed normal CBF and CVR were not bypassed, and there were no ischemic events in the mean 24-month follow-up. Of the nine patients with normal CBF but impaired CVR, eight were bypassed, and they showed no ischemic event and return of normal CVR on follow-up imaging. The one patient with poor CVR and without bypass suffered a CVA. Of the 11 patients with decreased baseline CBF and poor CVR, nine had bypass—of these, one suffered a perioperative CVA, one died of pneumonia, and CVR normalized in the rest with no further ischemic events. Of the two not bypassed, one suffered a CVA, and one had progressive deterioration followed by a basal ganglia hemorrhage. The final group consisted of patients with decreased baseline CBF, but normal CVR. Five of six were bypassed and none had subsequent CVA. The authors suggested that this may not, in fact, have represented a high-risk group, and that metabolic data may have shown decreased tissue metabolic demand.29 This study, although somewhat complicated and clearly limited due to the nonrandomized nature, seems to offer supportive evidence that normal CVR is protective, decreased CVR has a high rate of stroke when untreated (all three patients in this series), and bypass seems to offer significant protection from CVA with some risk of significant perioperative complications (two of 22 in this series).
A larger series looking specifically at this at-risk group based on decreased CVR followed again from the Pittsburg group.30 Forty-two patients with hemodynamic insufficiency were examined (baseline CBF < 45 cc/100 g/min and >5% negative reactivity). Thirty were treated medically and there were nine (30%) CVAs within 12 months (mean of 5 months). Twelve were bypassed only after developing an ischemic stroke and showed normalization of CVR in all, and there was no CVA in the 18-month follow-up with one asymptomatic hemorrhage. This was further strong evidence for both the dangerous natural history of these patients and the ability of bypass to not only reverse the hemodynamic findings, but decrease CVA risk with a very low risk of morbidity.30
Related posts:
 Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
Radial Artery Harvest for Cerebral Revascularization: Technical Pearls
 Exploring New Frontiers: Endovascular Treatment of the Occluded ICA
Exploring New Frontiers: Endovascular Treatment of the Occluded ICA
 EC-IC Bypass for Posterior Circulation Ischemia
EC-IC Bypass for Posterior Circulation Ischemia
 Surgical Anatomy of EC-IC Bypass Procedures
Surgical Anatomy of EC-IC Bypass Procedures
 EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
EC-IC and IC-IC Bypass for Giant Aneurysms Using the ELANA Technique
 Decision Making in Cerebral Revascularization Surgery Using Intraoperative CBF Measurements
Decision Making in Cerebral Revascularization Surgery Using Intraoperative CBF Measurements
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


