Variations in Arterial Anatomy
Introduction
MDCTA offers a new appreciation of arterial and venous anatomy. All arteries and veins will show complete ‘filling’ or enhancement which, if the protocol is correctly timed, gives effective blood pool imaging. MDCTA therefore does not suffer from flow effects which can cause artifact in both magnetic resonance angiography (MRA) and DSA. With catheter DSA, dilution in a vessel due to the influx of blood not opacified by contrast agent limits its value in anatomical demonstration. This is most commonly illustrated in the complete assessment of the anterior communicating arterial complex in the Circle of Willis, which requires bilateral selective carotid catheterization with or without contralateral carotid compression with DSA, and even then may fail to demonstrate the complete anatomy. Conversely, if flow information is important, then MDCTA is not the ideal choice. Information about likely flow direction can only be inferred from MDCTA.
The ability to rotate a three dimensional angiographic image in any direction enables determination, for example, of the completeness of the Circle of Willis, the optimal view in which to coil an aneurysm, what a surgeon will meet on the approach to an aneurysm or an AVM. Many of the projections available with MIP and 3D CTA are not possible with standard biplane DSA. This facility also makes it easier to appreciate arterial fenestrations (partial fusions remaining from earlier embryological situations), and other common and uncommon vascular variations. The details of the acquisition angiographic techniques will be found in Chapters 8 and 9. Anatomical examples are given here and others are listed and identified as incidental in other chapters. Some anatomical variations will influence the manifestations of disease, e.g. if the posterior cerebral artery arises from the carotid and not the basilar artery as is usual, then carotid atheroma could cause occipital infarction.
Included are examples of anomalies for the great vessels, the cervical carotid and vertebrobasilar systems, in addition to intracranial variations.
Illustrations
Vascular variations are seen routinely as the number of noninvasive vascular studies keeps increasing, expanding our exposure to many more vessels than we had seen with catheter angiography or from earlier pathological studies. Some examples are included, all obtained from standard MDCTA techniques.
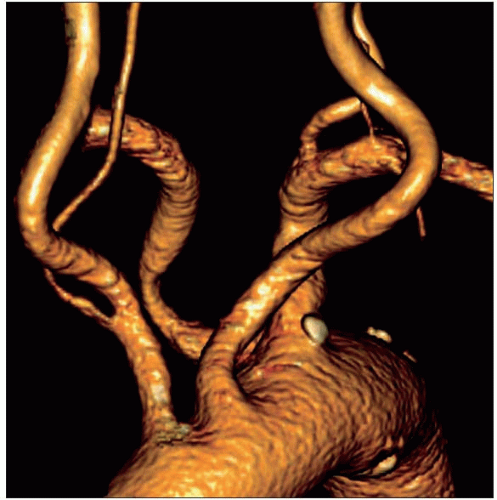 10.1 The right vertebral artery arises unusually from the right common carotid artery and there is an aberrant right subclavian arising distal to the left subclavian artery. |
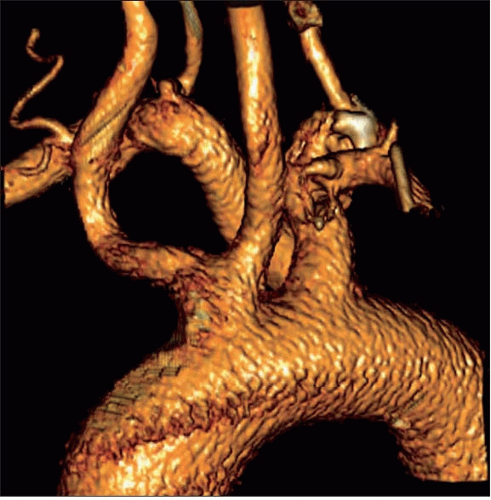 10.2 The aberrant right subclavian here gives rise to the right vertebral artery and there is a common origin of the right and left common carotid arteries. |
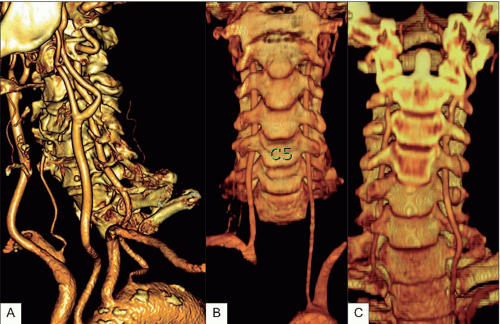 10.3 (A) The left vertebral artery arises directly from the aortic arch proximal to the left subclavian in about 5% of people; however, here it arises unusually beyond the left subclavian. This vertebral artery enters the vertebral canal at the usual level of C6, however the nondominant right vertebral enters at C4. (B) Both vertebral arteries enter the canals at C5, the left arising directly from the arch proximal to the left subclavian origin. (C) Here the right vertebral enters the canal at C6 and the left at C4. The proximal vertebral arteries are therefore very variable but this is not associated with any pathology.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





