Vascular Malformations of the Spine
Key Points
All of the available sources of supply to the anterior spinal artery may not declare themselves readily on the initial angiographic evaluation. Care should always be exercised when using particulate or liquid agents near the spinal cord, lest an unsuspected pedicle to the anterior spinal artery be present.
Manifestations of spinal venous hypertension may be very subtle, particularly on nonenhanced MRI examinations.
Introduction
Spinal cord vascular malformations represent about 2% to 3% of spinal masses and typically present with myelopathic symptoms related to compromise of long tract function (bowel and bladder dysfunctions, motor and sensory losses) but can also present with back pain, radicular symptoms, subarachnoid or intraspinal hemorrhage, or spinal deformity.
Spinal arteriovenous malformations are rare. With the exception of spinal dural arteriovenous malformations, there are probably almost as many publications and classification systems for spinal vascular disease in the literature as there are patients with these disorders. The most helpful way to understand these lesions is by their location with reference to the dura and the spinal cord. Secondarily, they can be categorized into simple fistulous lesions (AVF) or multivessel lesions (AVM). Intramedullary AVMs are classified into juvenile type (whole cross-sectional area of the cord involved) or glomus type (a more restricted pea-like configuration). Pial fistulas are usually on the surface of the cord or just below and are sometimes graded according to the degree or absence of ectasia of the feeding arteries.
Spinal AVMs can alternatively be classified from a genetic point of view:
Genetic hereditary lesions of the vascular germinal cells, such as seen in hereditary hemorrhagic telangiectasia.
Genetic nonhereditary lesions with metameric expression, such as Cobb syndrome where patients have multiple shunts and malformations of the spine, muscles, paraspinal and cutaneous tissues.
Dural arteriovenous fistulas, on the other hand, are tiny, slowly flowing lesions, which with rare exceptions represent an acquired disease of later adulthood (>40 years). They are supplied by dural arteries and typically affect the lower spine and lower extremities. They cause a more progressive slow decline compared with intramedullary vascular malformations. They do not typically cause subarachnoid hemorrhage.
Intradural Spinal Arteriovenous Malformations
Intradural, intramedullary spinal arteriovenous malformations occur most commonly in the cervical or thoracic cord and are classified into three types (Figs. 21-1–21-5).
Juvenile-type Spinal Arteriovenous Malformations
The juvenile type of spinal arteriovenous malformations occupies the entire spinal canal at the involved level(s) and can have normal spinal parenchyma present within the interstices of its components. There may be multiple medullary arterial feeders, most prominently the anterior spinal artery, which, like the arterial feeders to arteriovenous malformations in the brain, may have a dysplastic appearance. Feeding pedicle or intranidal aneurysms may be seen in approximately 20% of intramedullary arteriovenous malformations (3,4), as can venous ectasia or venous aneurysms. A minority of patients show a widened interpedicular distance and may even emit an audible spinal bruit (Fig. 21-6). They can present with gradual or abrupt onset of motor and sensory symptoms related to the level of involvement or with spinal subarachnoid hemorrhage.
Glomus-type Spinal Arteriovenous Malformations
Glomus-type spinal arteriovenous malformations are more compact and defined than the juvenile type. They do not have intermingled normal spinal tissue, are confined to a shorter segment of cord, and are usually fed by a single arterial pedicle. They have a risk of subarachnoid hemorrhage higher than that of other types of intradural vascular malformations, seen in 85% of symptomatic patients (3).
Intramedullary and Perimedullary Arteriovenous Fistulas
Fistulas of the spinal cord may be intramedullary or perimedullary. Flow is usually from an anterior or posterior
spinal artery, which connects directly to a vein without an identifiable nidus. Flow is faster than that seen in dural arteriovenous fistulas. They can present with intramedullary or subarachnoid hemorrhage, but this appears to be a minority of cases. As is the case for dural arteriovenous fistulas, venous hypertension with cord edema appears to be an important pathophysiologic mechanism for symptoms of intradural arteriovenous shunts (5). Aneurysms of the feeding pedicles are not as likely to be present with perimedullary fistulas compared with intramedullary arteriovenous malformations (4).
spinal artery, which connects directly to a vein without an identifiable nidus. Flow is faster than that seen in dural arteriovenous fistulas. They can present with intramedullary or subarachnoid hemorrhage, but this appears to be a minority of cases. As is the case for dural arteriovenous fistulas, venous hypertension with cord edema appears to be an important pathophysiologic mechanism for symptoms of intradural arteriovenous shunts (5). Aneurysms of the feeding pedicles are not as likely to be present with perimedullary fistulas compared with intramedullary arteriovenous malformations (4).
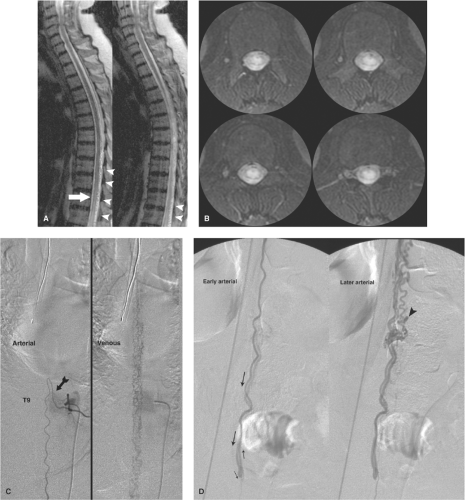 Figure 21-1. (A–D) Intramedullary spinal arteriovenous malformation presenting with venous infarction (Foix–Alajouanine). A 53-year-old female presented with a 3- to 4-year history of progressive lower extremity weakness, incontinence, and ascending sensory disturbances. Her presentation was confounded by a remote history of surgical release of a tethered cord. However, her sagittal (A) and axial (B) T2-weighted MRI images at the time of presentation show findings not likely related to the previous surgery. The conus is hyperintense in signal (arrow), and numerous flow voids (arrowheads) are seen along the dorsal surface. The axial appearance is that of a “hyper-round” cord, which could be seen with an arterial infarction of the artery of Adamkiewicz or a tumor of the conus. In this instance, however, the appearance is that of a venous infarction with chronic venous hypertension in the lower cord. This could be due to either a dural AVF along the cord or a pial AVM on or in the cord itself. The diagnostic spinal arteriogram must find and analyze the lesion accordingly in order to plan treatment. In this particular patient, the lesion was an intramedullary arteriovenous malformation of the cord deriving supply from the anterior spinal artery. This vessel was found at left T9 (arrow in C) and was injected (2mL/s × 2s) with the intensifier centered over the catheter tip as shown. The arterial phase was significant for marked conspicuity of the anterior spinal artery, implying that it was enlarged, but was otherwise normal. However, the venous phase demonstrates that the venous plexus of the cord is markedly distended and exhibits prolonged stagnation. This is an illustration of the importance of the entire angiographic sequence for critical vessels. A subsequent run centered over the conus (D) shows that the arteriovenous malformation is located on the dorsum of the cord. The anterior spinal artery descends along the anterior median sulcus, wraps around the tip of the conus—centered at L3 in this patient—and ascends the dorsum of the cord to opacify the arteriovenous malformation (arrows indicate sequential progress of flow). An intranidal aneurysm is noted (arrowhead in D). The venous structures then emanate cephalad to allow eventually the opacification seen on image (C). Technique is very important in spinal angiography because the findings can be so elusive that they can easily escape attention due to oversight or technical shortfalls. |
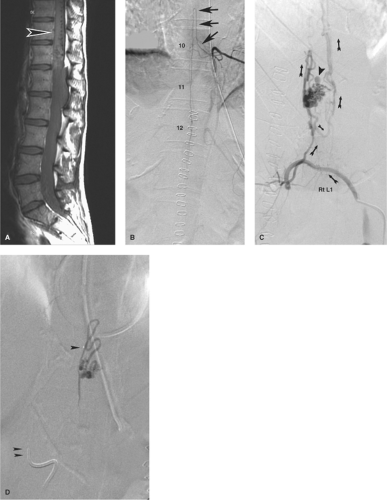 Figure 21-2. (A–D) Intramedullary spinal arteriovenous malformation presenting with intraconal hemorrhage. When this young patient collapsed in a setting of courtroom stress and became paralyzed from the waist down, it seemed to be a textbook example of a hysterical conversion disorder. However, her MRI showed a large intraconal hemorrhage, which was evacuated emergently. A postoperative sagittal MRI (A) revealed a profusion of flow voids on the dorsum of the conus (arrowhead in A), which had not been seen on the preoperative scan. In contrast to that shown in Figure 21-1, the anterior spinal artery at left T10 (arrows in B) has a more normal appearance with no pathologic venous opacification seen. The offending lesion is an arteriovenous malformation of the surface of the cord found on the right L1 injection (C, oblique view with arrows showing sequence of flow). An intranidal aneurysm, which is likely the site of hemorrhage, is noted (arrowhead in C ). The postembolization roadmap view (D) shows the ease with which inadvertent reflux of liquid embolic agent can occur when one is attempting to perfuse the nidus of a lesion. In this instance, there was a presumed safety margin between the microcatheter tip (single arrowhead in D) and the main catheter tip (double arrowhead in D) at the aortic wall, but as a general rule, relying on such landmarks is not foolproof. Reflux of liquid could permeate adjacent segmental arteries through collateral pathways with unintended results. |
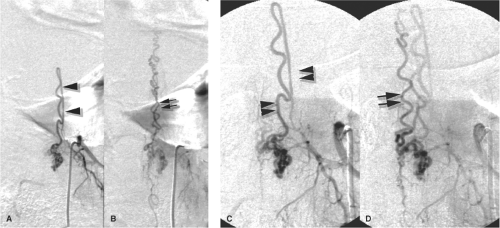 Figure 21-3. (A–D) Perimedullary spinal arteriovenous malformation. An elderly male presented with a clinical history of gait disturbance and urinary incontinence. MRI and myelographic findings (not shown) suggested spinal venous hypertension. A left T12 injection demonstrates an enlarged posterior spinal artery (arrowheads in A) supplying a perimedullary arteriovenous malformation of the surface of the cord. The early venous phase of the PA view (B) shows drainage of the arteriovenous malformation superiorly through the tortuous venous plexus of the spine. An oblique magnification view of the same pedicle (C, early; D, late) helps to clarify the surgical anatomy. The posterior spinal artery (arrowheads in C) behind the cord makes a hairpin turn on the posterior surface to supply the perimedullary nidus. A slightly later image (D), taken when the posterior spinal artery is almost washed out, demonstrates the most prominent vein (double arrow in D) draining along the surface of the cord. |
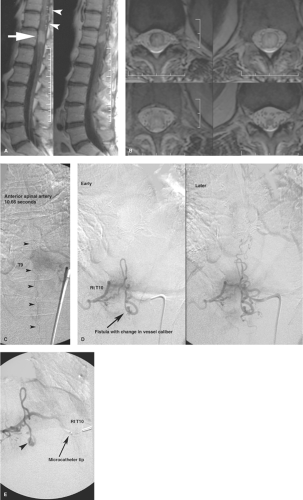 Figure 21-4. (A–E) Spinal arteriovenous malformation with venous hypertension (Foix–Alajouanine) mimicking a conal mass. An 83-year-old female with a remote history of breast carcinoma presented with progressive lower extremity weakness and sensory disturbance. An enhancing mass on her sagittal T1 gadolinium-enhanced MRI (arrow in A) prompted the diagnosis of metastatic carcinoma to the cord. The axial T2 MRI (B) seemed to confirm the expansile hyperintense appearance of the cord. However, she had no other history of metastatic disease, and a prominence of vascular structures (arrowheads in A) on the dorsum of the cord suggested that an arteriovenous malformation might be a consideration. The anterior spinal artery at left T9 shows indirect signs of disease. In this case, the anterior spinal artery (C) is struggling to perfuse the cord against a state of venous hypertension. However, because the anterior spinal artery is not a route of supply to the arteriovenous malformation, it is normal in size but very stagnant in its circulation. At 10.66 seconds following a 2-second injection, it remains opacified and slowly flowing (arrowheads in C). This is an important finding in the course of a spinal angiogram, as it can prompt the operator to be aware that there is definitely something wrong with the arteriovenous gradient in the cord. The offending lesion is seen at right T10 (D) with a very small nidus and immediate opacification of the venous plexus. A magnification view (E) via the microcatheter shows the change in vessel caliber (arrowhead in E), which is a very good angiographic sign for the precise point of any fistula. |
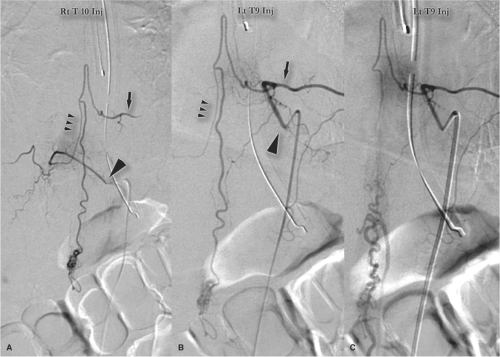 Figure 21-5. (A–C) Be wary of unexpected anatomic variants in the anterior spinal artery. These images from the diagnostic evaluation of a perimedullary AVM or fistula on the dorsum of the conus illustrate the variability of the input to the anterior spinal artery. The right T10 injection (A) catheter tip indicated with arrowhead) shows a small pedicle (triple arrowhead in A) extending up to the midline, with retrograde reflux to the larger contributor to the anterior spinal axis from left T9 (arrow in A). The subsequent direct injection of left T9 (B) shows the same anatomy, with a slightly different emphasis in conspicuity. A slightly later image (C) demonstrates the centrifugal veins emanating from the region of the AVM extending caudad along the lumbar nerve roots. The images from this case are relatively clear in what they demonstrate but are selected here to make the point that the anatomy of the anterior spinal axis can be very unpredictable, and may even have seemingly redundant feeders. In some circumstances these can pose a substantial risk for misadventure through particle or liquid embolization of unexpected pedicles. |
Paraspinal and Epidural Arteriovenous Malformations
Paraspinal AVMs are rare lesions that can affect the paravertebral muscles, nerve root foramina, or prevertebral structures (6). They can be seen posttraumatically, but most are considered to be congenital lesions presenting in children with back pain, paraparesis, high-output cardiac failure, or an audible bruit (Fig. 21-7). Most of them seem to exert their functional effect through venous congestion transmitted to the intradural veins.
Hypervascular Tumors Simulating Arteriovenous Malformations
Arteriovenous shunting or early venous opacification can be seen with vascular intra-axial tumors such as glioblastoma multiforme (Figs. 21-8 and 21-9) or hemangioblastoma. Extra-axial vascular tumors, such as hemangiopericytoma and extra-axial or spinal hemangioblastoma, may also give an appearance that could be confused with that of an arteriovenous malformation. Usually, the vascularity of such tumors is easily recognized as subordinate in prominence to other evidence of a mass lesion. Arteriovenous shunting is rarely as fast in a tumor as that seen in arteriovenous malformations. A parenchymal blush characteristically seen in vascular tumors is not seen in arteriovenous malformations.
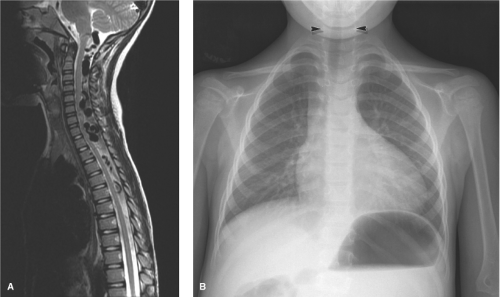 Figure 21-6. (A–B) Syndromic spinal AVM in a small child. This presumably congenital AVM of the cervical spine was characterized by a number of high-flow fistulas that had resulted in massive distention of the veins of the spinal cord draining upward via the foramen magnum (A). In fact the distended appearance of the basal vein of Rosenthal and mesencephalic veins gave the appearance at first glance that this might be a vein of Galen type of malformation in the tectal region, until one realized the fact that these veins were emerging out of the spinal canal into the cranial vault, instead of vice versa. The chest x-ray in this child (B), who had an audible bruit over his neck and suboccipital area, shows the widened interpedicular distance (arrowheads) wrought by such lesions when they occur early in development. |
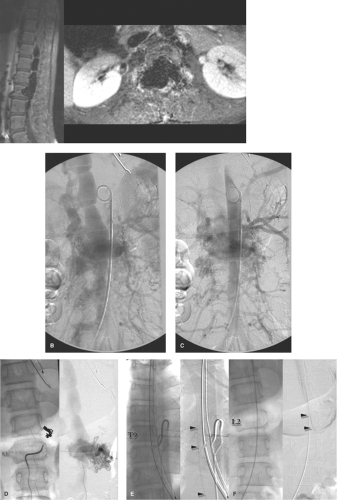 Figure 21-7. (A–E) Paraspinal AVM in a young child. This girl presented with high-output cardiac failure, a bruit over the lower back, and scoliotic deformity. Her cardiologist astutely noted that the contrast from her ventriculogram returned to the heart more quickly than normal, leading to the eventual discovery of this large lumbar paraspinal malformation. The treatment for this lesion predated the availability of Onyx and was staged over several years. The initial MRI (A) showed massive distension of the intracanalicular veins and permeative remodeling of the lumbar bodies, particularly L2. The first aortogram AP projection (image B early, image C venous) shows the numerous enlarged lumbar and paraspinal arteries involved with this lesion, and the massively enlarged intracanalicular vein that ascended to enter the azygous vein in the thorax. Among the many concerns with this child who is obviously in need of significant reduction of flow in this lesion is where to begin and how to embolize this lesion without injuring the anterior spinal artery? Image (D) places native and subtracted views from the left L2 injection side by side during the initial tentative embolization using coils in some of the direct fistulas. A large component of AVM is opacified from left L2 draining immediately to the intracanalicular vein. A different set of images indicates the hidden dangers that can lurk in cases like these. The left T9 injection (E, native and subtracted) demonstrates the normal-sized anterior spinal artery (arrowheads), which takes an unusual sweep toward the left as it descends along the cord, perhaps reflecting displacement by the massive vein within the canal. A second image (F, native and subtracted) with the catheter still in Left T9 but centered lower over L2 shows that mass effect is not the entire explanation. The anterior spinal artery bevels away from the cord itself and descends to the left L2–L3 foramen and then is cut off at a precise point. The image is telling us that there is a major input to the anterior spinal axis at left L2, but it has become reversed due to the sump effect of the AVM. In other words, the anterior spinal axis is supplying the AVM with flow (to a small degree) through the reversed L2 ramus. One needs to be very careful with this discovery. A sudden, effective embolization of left L2 (or even some of its immediate neighbors) with a liquid agent could eliminate the sump of the AVM in this local area, causing the left L2 ramus to the anterior spinal artery to reverse itself suddenly. This could result in transmission of liquid agent to the cord. |
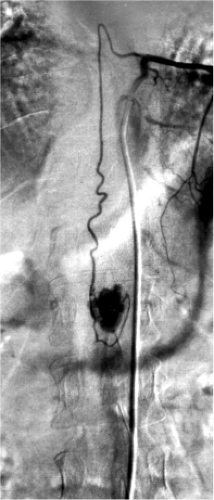 Figure 21-8. Spinal hemangioblastoma. A patient with Von Hippel–Lindau syndrome and multiple hemangioblastomas of the posterior fossa and cervical spine. A tumor of the lumbar spine opacified via the anterior spinal artery from left T8 injection is demonstrated. Hemangioblastomas typically give a dense immediate blush that reaches prominence during the early arterial phase of an injection, and are thus easily distinguished from vascular malformations. |
Endovascular Treatment of Spinal Vascular Malformations
The prognosis for an untreated symptomatic spinal AVM is poor with 36% of patients younger than 40 years progressing to severe impairment of function within 3 years (7). Safe endovascular embolization of spinal vascular lesions hinges on the ability to distinguish between a posterior spinal artery and an anterior spinal artery. Typically an average-sized PSA supplies a small rim of peripheral tissue centripetally in the posterior third of the cord and its loss, inadvertent or otherwise, is thought to be well tolerated due to the proclivity to develop collateral pathways of supply (8). The anterior spinal artery is a different story. Typically it supplies the greater portion of the cross-sectional territory of the spine at any one level due to penetrating branches from the anterior median sulcus, the sulco-commissural branches, which measure between 400 and 100 μm in size (9) tapering to approximately 60 μm as they penetrate the cord parenchyma centrifugally (10).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


