♦ Preoperative
Operative Planning
- Review imaging (computed tomography [CT] or magnetic resonance imaging)
- Measure and record radiographic distance on chest x-ray from clavicle to the junction of superior vena cava and the right atrium
- Placement of ventricular catheter
- We prefer occipital placement on the right side
- If there is marked asymmetry of the ventricles, the left side and/or frontal placement may be used
- We prefer occipital placement on the right side
- Distal catheter placement: consider general or pediatric surgeon assistance for complex cases
Equipment
- Basic shunt tray
- Shunt system
- Controversy about correct shunt valve exists given new technology and pending results from ongoing multicenter trials.
- We preferentially use an adjustable flow control valve (PS-Medical Strata valve, Medtronic) in older children and adults.
- In newborn and infants, a low- or medium-pressure flow controlled shunt system (PS-Medical Delta valve, Medtronic) is preferred.
- Valve connected 1.5 to 2.0 cm from burr hole to allow revisions via a single incision
- In newborn and infants, a low- or medium-pressure flow controlled shunt system (PS-Medical Delta valve, Medtronic) is preferred.
- Controversy about correct shunt valve exists given new technology and pending results from ongoing multicenter trials.
- Venous access: a Broviac or Hickman catheter kit (Davol, Cranston, RI) may be opened with the following equipment used
- An introducer needle
- A 5 or 10 mL syringe
- A guide wire
- A Peel-Apart introducer (Bard Access Systems, Salt Lake City, UT) with vessel dilator
- An introducer needle
Operating Room Set-up
- Headlight
- Loupes (optional)
- Bipolar cautery and Bovie cautery
Anesthetic Issues
- General anesthesia
- Normothermia shuold be ensured with warm temperature, disposable heat-controlled blankets, and/or heat lamps for infants.
- Intravenous antibiotics with skin flora coverage (cefazolin 2 g for adults, 30 mg/kg pediatrics) shuold be given within 30 minutes prior to skin incision.
- Degree of intracranial pressure elevation shuold be communicated to anesthesiologist.
♦ Intraoperative
Positioning
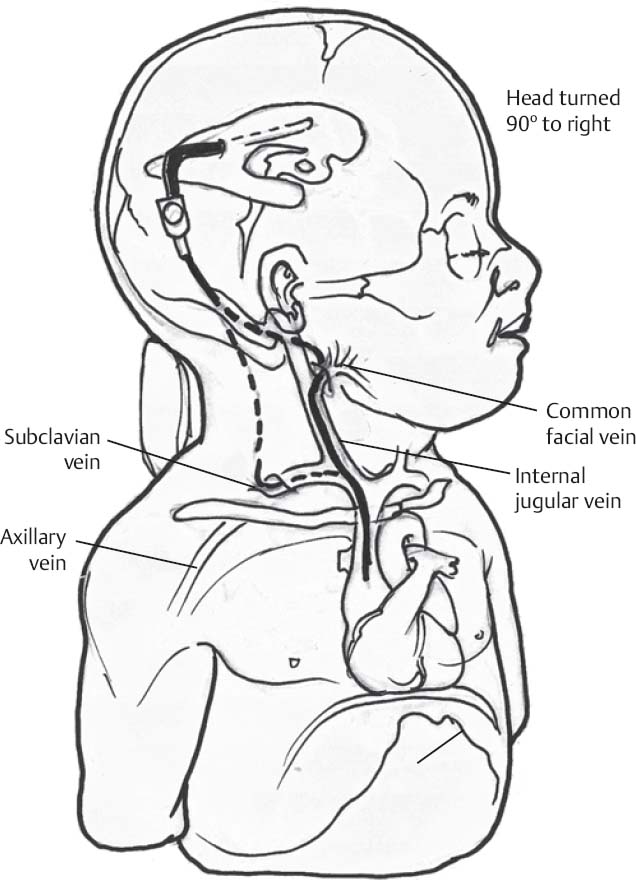
- Patient’s head turned 90 degrees to opposite side if no contraindications
- Neck elevated slightly with pads or shuolder roll
- Eyes secured shut
- Heels and ulnar areas padded
Planning of Shave
- Use disposable hair clippers
- Width is two fingerbreadths in a child, three fingerbreadths in an adult
- Some surgeons prefer only area around incision shaved, others include shunt tract path
Planning of Incisions
- Scalp: crescentic, 3 cm curvilinear incision with a dot 1 cm within incision line marked for burr hole placement
- Cervical: using ultrasound guidance the internal jugular vein shuold be located ~4 cm superior to clavicle and a 1.5 to 2 cm horizontal line marked over this location
- Old incisions shuold be reused when possible
- Five-minute scrub is performed using either a moistened chlorhexidine scrub brush or a Betadine detergent scrub
- Sterile towel completely dry
- Apply DuraPrep and allow 3 minutes to dry or alternatively apply a Betadine paint
- Apply Ioban drapes over exposed head, neck, chest, and abdomen
- Always prep the abdomen and chest in case an alternate distal location needs to be used
Shunt Assembly
- Shunt valve shuold be attached to distal catheter and secured with a 2–0 silk tie
- The catheter shuold be primed in normal saline with bibiotic solution ensuring distal flow
- The partially assembled system is then placed in normal saline with bibiotic solution
Scalp Incision
- A curvilinear, semilunar incision is made to create a pocket within the confines of the incision
- Linear incision carries a higher risk of damage to the shunt valve or system if revision is required in the future
- Small, self retaining Weitlaner retractor is placed
Burr Hole
- Occipital approach
- Three cm behind and 3 cm above ear (may be estimated with fingerbreadths)
Cervical Approach
- Incision through the skin and Bovie cautery through subcutaneous tissue
- Platysma divided sharply (Metzenbaum scissors or no. 10 blade)
Shunt Pass
- Advance bent passer, usually from below; we prefer metal passers because catheters are less likely to stick
- Single pass for occipital placement
- Additional retroauricular incision is usually necessary for frontal placement
- Pocket for valve is created by lifting shunt passer and dissecting underneath using Bovie cautery to a depth of ~5 cm from burr hole
- Distal tubing is tied to the end of the shunt passer using 2–0 silk ligature
- Passer is withdrawn to pass distal shunt tubing subcutaneously from cranial to cervical incision
- Ensure 1 to 2 cm distance from burr hole to shunt valve
Proximal Catheter Placement
Only gold members can continue reading. Log In or Register to continue




