44 Vessel-X
KEY POINTS
Introduction
Since vertebroplasty was introduced by Herve and Deramond in 1984, many methods of percutaneous osteoplasty (molding the bone) evolved to treat symptomatic vertebral compression fractures (VCFs), by injection of bone filler material (BFM): polymethylmethacrylate (PMMA), other kinds of bone cement, and bone grafts (autografts and allografts), or different kinds of osteoinductive or osteoconductive materials. The same risk in performing the previously mentioned techniques is the leakage of BFM, because the injected pressure will go to the fracture’s weakest area and lead to a leakage. Vesselplasty is an osteoplasty technique using the Vessel-X, which acts as an implant body expander to restore vertebral height in VCFs but prevents the potential risk of leakage.1,2
Indications and Contraindications
Indications
The procedure is indicated for symptomatic VCFs in the thoracic or lumbar vertebrae stemming from2:
Description of the Device
The idea behind the prototype originated in Taiwan, in February 2002 (Figure 44-1). The cadaveric study using the prototype was done by the author in Jakarta, Indonesia, in July 2003. The first generation used in the clinic was named threadplasty, because the connection used was thread (Figure 44-2).


A clinical trial was done in Jakarta, Indonesia, by the author from July 2004 until July 2005. As a preliminary report the first three cases were presented at the Asia Pacific Orthopaedic Association (APOA) Triennial Meeting in Kuala Lumpur on September 5-10, 2004. After the ten first-generation vesselplasty devices (Threadplasty) were made and during the clinical trial, major improvements and developments were made to formulate the last-generation instruments available for clinical use (Figure 44-3).1–6

Vessel-X is a bone filler container made of polyethylene terephthalate (PET), a nonstretchable material. In deflated condition its shape is long, and when it is inflated the shape becomes short and bigger until a certain size is reached. When the pressure inside the container is equal to the surrounding resistance, the final size is achieved and the size will remain constant. This mechanical device is used to lift the vertebral endplate, acting like an implant body expander (Figure 44-4).

The Vessel-X container is a PET mesh and has 100-μm porosity. When the pressure inside the container is greater than the surrounding resistance, the BFM starts to interdigitate through the pores; some pressure is then relieved and the endplate is lifted further (Figures 44-5 and 44-6).

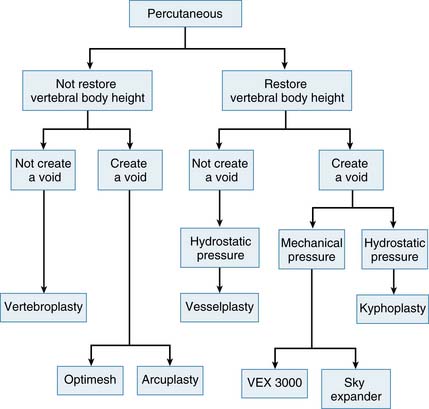
The Variations in technical concepts in percutaneous osteoplasty have led to the differences in techniques and results for the numerous methods: vesselplasty (KYPHON INC. CA), vertebroplasty, kyphoplasty, VEX-3000 (Taeyeon Medical CO., LTD, South Korea), Sky Expander (DISC-O-TECH MEDICAL TECHNOLOGIES, LTD., IS), arcuplasty (Warsaw Orthopedic, Inc, IN), and the Optimesh system (Spineology, Inc., MN) (Figure 44-7). Vertebroplasty is not used to restore the vertebral body height (VBH), whereas the other techniques are accomplishing the same goal by first creating a void. The other concepts do restore VBH and create a void by mechanical or hydrostatic pressure. The difference between the restoring VBH group is based on the technical methods and instruments to lift the vertebral endplate. To restore VBH, all techniques except vesselplasty need to first create a void by mechanical or hydrostatic pressure, followed by filling the void with PMMA or other BFM. All the previously mentioned techniques carry different risks of leakage, because if the BFM is injected directly into the bone or void, it will go to the weakest fracture area. The vesselplasty technique requires only that a hole be drilled into the vertebral body as a place to be occupied by the deflated PET container (almost like screw insertion into the bone). Then the container is inflated by injecting viscous PMMA or other BFM, and the hydrostatic pressure lifts the vertebral endplate, acting as an implanted vertebral body expander.1,6–16
Sequential injection of BFM into a nonstretchable container will prevent leakage, because inside the container the pressure will be distributed equally to all direction. Under a continuous sequential injection the pressure is released outside the Vessel-X through the pores sequentially, because the container size is constant, and starting the interdigitation works like vertebroplasty. The sequential pressure release and the interdigitation will further lift the endplate yet still preventing leakage, because the pressure is equally distributed in all directions. The most important point is the experienced surgeon’s judgment of when to end the procedure, which is related to the individual patient’s condition (Figures 44-8 and 44-9).

Background of Scientific Testing and Clinical Outcomes
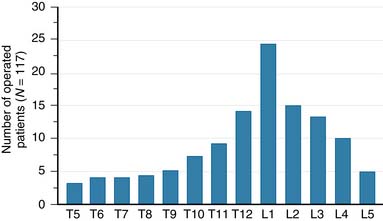
A nonrandomized 3-year prospective follow-up study on 103 patients who had single- or multiple-level stable VCFs from T5 to L5, involving a total of 117 vertebrae (Figure 44-10). In 86 cases, fractures were in osteoporotic vertebrae, compared to 17 cases where the fractures were due to high energy trauma. The number of females, 69 cases, was twice the number of males, at 34 cases. The average patient age was 70.3 years, with the youngest 34 years old and the oldest 98 years old. Fracture age ranged from 1 day to 70 days after the trauma.
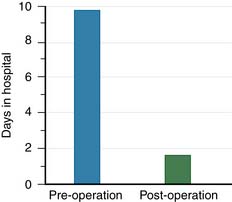
One day after treatment, all patients gained significant pain relief, as determined from the VAS, which dropped from 9.9 to 1.7 (p < .001), and the average hospital stay was 2.2 days (Figure 44-11). The average vertebral height restoration was 96.4% (range, 100% to 50%) related to the variable bone density from old to young patients, fracture type, and fracture age. A variable amount of BFM was injected into the small 20-mm Vessel-X, from 2.5 ml to 10.25 ml, without any leakage, bleeding, or neurologic deficits, and only two adjacent level fractures were detected 1 year after treatment on the eldest patients, who were older than 90 years.
Case Studies




CASE 3 (2007) (Figures 44-16 and 44-17)

Related posts:
 Embryology of the Spine
Embryology of the Spine
 Non-Invasive Strength Analysis of the Spine Using Clinical CT Scans
Non-Invasive Strength Analysis of the Spine Using Clinical CT Scans
 Tumors of the Cervical Spine
Tumors of the Cervical Spine
 Rheumatoid Arthritis of the Cervical Spine
Rheumatoid Arthritis of the Cervical Spine
 The Role of Spinal Fusion and the Aging Spine: Stenosis without Deformity
The Role of Spinal Fusion and the Aging Spine: Stenosis without Deformity
 The Role of Spinal Fusion and the Aging Spine: Stenosis with Deformity
The Role of Spinal Fusion and the Aging Spine: Stenosis with Deformity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


