Voluntary and Involuntary Movements in Humans
Mark Hallett
ABSTRACT
Psychogenic movements may be voluntary or involuntary. If voluntary, the mechanism is factitious or malingering and the patient is lying. Most commonly, the movements are conversion or somatization in origin, and are involuntary. The movements look voluntary, however, and the fact that they are preceded by a normal-looking Bereitschaftspotential suggests that they share some brain mechanisms with normal voluntary movement. Perhaps there is an unconscious force that initiates these movements. More likely, the brain just does not interpret them as being voluntary. There is good evidence that the brain generates movements as a result of all the inputs to the motor system, and that the sense of voluntariness is a perception. Physiologic studies are providing information on how this can happen.
INTRODUCTION
Psychogenic movement disorders may be factitious or malingering. In these circumstances, the movement is voluntary, but the patient says it is involuntary. The patient is lying. The task for the physician is to determine that the patient is lying, and this is not necessarily easy. All agree that the lie detector test is not foolproof. There has been some work in this area using electroencephalogram (EEG) and functional magnetic resonance imaging (fMRI) (1, 2, 3, 4), but there is nothing definitive yet, certainly on the individual level. More work is needed in this area of investigation, and this problem will not be considered further in this chapter. However, whether the patient is lying or not is really the first consideration when faced with a patient with psychogenic movements.
Most patients with psychogenic movement disorders have a conversion etiology. The mechanism of somatization is thought also to be conversion. Patients with conversion exhibit movements that look voluntary and even share some physiologic aspects with voluntary movements, but the patients say that the movements are involuntary. In general, we believe this to be true. Indeed, if the patient was lying, and the movements were actually voluntary, we would make a different diagnosis. These considerations raise a number of questions. Are the patients just lying to themselves, and if so, what does that mean? What makes a movement voluntary? What separates voluntary and involuntary movements?
Clearly the critical aspect of voluntary movement is that a person believes that he or she has chosen to make the movement. This is the general view of free will, the decision to make (or not make) movements. The brain is certainly responsible for all movements that the body makes. Only a subset is thought to be voluntary. The “thought of voluntariness” is a qualia of consciousness (5), an element of which a person is aware. The nature of consciousness is a difficult matter and dealt with elsewhere in this book (see Chapter 24). Is it the case that movements are actually “chosen,” or is the “choosing” just a perception of
consciousness? This issue will be addressed here, but also elsewhere in this book (see Chapters 23 and 24).
consciousness? This issue will be addressed here, but also elsewhere in this book (see Chapters 23 and 24).
ARGUMENTS IN FAVOR OF FREE WILL AS A PERCEPTION
One possibility is that there is some mechanism in the brain that chooses the movement to be made. This is certainly the commonly held view. On the other hand, there are several arguments that can be made that the brain’s motor system produces a movement as a product of its different inputs, consciousness is informed of this movement, and it is perceived as being freely chosen. It is controversial which of these is correct, but there are some good arguments in favor of the latter.
The Brain Initiates a Movement before Awareness of Volition
The clever experiment that showed this was reported by Libet et al. in 1983 (6). Subjects sat in front of a clock on which a rapidly moving spot was projected and were told to move at will. Subsequently, they were asked to say what time it was (where the spot was) when they had the first subjective experience of intending to act (this time was called W). They also were asked to specify the time of awareness of actually moving (this time was called M). There were two types of voluntary movements: one type was thoughtfully initiated and a second type was “spontaneous and capricious.” As a control for the ability to successfully subjectively time events, subjects were also stimulated at random times with a skin stimulus and they were asked to time this event (called S). At the same time, EEG was being recorded and movement-related cortical potentials (MRCPs) were assessed to determine timing of activity of the brain.
The MRCP has a number of components (7). An early negativity preceding movement has two phases: an initial, slowly rising phase lasting from about 1,500 ms to about 400 ms before movement [the Bereitschaftspotential (BP), also called the readiness potential in translation of the German], and a later, more rapidly rising phase lasting from about 400 ms to approximately the time of movement onset, the negative slope, or NS’. (These two components could also be called the BP1 and the BP2.) The NS’ peaks about 90 ms before the onset of EMG activity and is followed often by a brief decline in the negativity, called the premotor positivity. The next component is the motor potential or MP which begins before movement, peaks after movement onset, and produces the highest negativity in the recording. The topography of the BP is generalized with a vertex maximum. With NS’, the negativity begins to shift to the central region contralateral to the hand that is moving. The main contributors to the BP are the primary sensorimotor cortex and premotor cortex, and the supplementary motor area, both bilaterally (8). With the appearance of NS’, the activity of the contralateral motor cortical regions predominate. With thoughtful, preplanned movements, the BP begins about 1,050 ms prior to electromyogram (EMG) onset (the type 1 of Libet), and with spontaneous movements, the BP begins about 575 ms prior to movement (the type 2 of Libet) (9). The type 2 may consist mainly of the NS’ component.
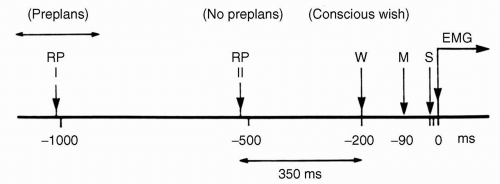 Figure 22.1 Timing of subjective events and the Bereitschaftspotential (readiness potential, RP) with data from Libet et al. (1983). RP1 is the onset of the Bereitschaftspotential with ordinarily voluntary movements and RP2 is the onset with movements made quickly with little forethought. W, the subjective timing of the will to move; M, the subjective timing of the onset of movement; S, the timing of a shock to the finger. Electromyogram (EMG) onset is set at 0 ms. (From Libet et al. Readiness-potentials preceding unrestricted “spontaneous” vs. preplanned voluntary acts. Electroencephalogr Clin Neurophysiol. 1982;54:322-335.) |
While the MRCP clearly is indicative of movement preparatory processes in the brain, its exact meaning is not clear. In particular, a relatively normal-looking MRCP precedes unconscious movements as well as conscious movements. This was studied by looking at the brain events preceding unrecognized movements made by subjects at rest or engaged in a mental task (10).
Subjects were reasonably accurate in determining the time of S, indicating that this method of timing of subjective experience was acceptable. W occurred about 300 ms prior to EMG onset, and M occurred about 90 ms prior to EMG onset. The onset of the BP type 1 occurred about 800 ms prior to W, and the onset of the BP type 2 occurred about 350 ms prior to W (Fig. 22.1). The authors concluded that
“cerebral initiation of a spontaneous, freely voluntary act can begin unconsciously, that is, before there is any (at least recallable) subjective awareness that a ‘decision’ to act has already been initiated cerebrally”(6).
“cerebral initiation of a spontaneous, freely voluntary act can begin unconsciously, that is, before there is any (at least recallable) subjective awareness that a ‘decision’ to act has already been initiated cerebrally”(6).
Voluntary Movements Can Be Triggered with Stimuli That are Not Perceived
To understand the experiments here, the phenomenon of backward masking is a prerequisite. By itself, a small stimulus would be easily recognized. If the small stimulus is followed quickly by a large stimulus, then only the large stimulus is appreciated; the small one has been masked. This phenomenon is robust and has been demonstrated in the visual and tactile modes. Its physiology is not completely understood, although there is some speculation (11).
Taylor and McCloskey (12) looked to see if voluntary movements could be triggered by backwardly masked stimuli. Large and small visual stimuli were presented to normal human subjects in two different experiments. In some trials, the small stimulus was followed 50 ms later by the large stimulus. In perception experiments, the researchers demonstrated in this circumstance that the small stimulus was not perceived even with forced-choice testing showing the phenomenon of “backward masking.” In reaction time (RT) experiments, the RTs for responses to the masked stimulus were the same as those for responses to the easily perceived, nonmasked stimulus. Hence, subjects were reacting to stimuli not perceived. In this circumstance, the order of events was stimulus-response-perception, and not stimulus-perception-response that would seem necessary for the ordinary view of free will.
Sense of Volition Depends on Sense of Causality
Wegner and Wheatley (13) point out that the experience of will depends on the relationship between one’s thought and the movement itself. The thought must occur before the movement, it must be consistent with the movement, and there must not be another obvious cause for the movement. These features that are aspects of causality imply that the thought led to the movement. Thus, the fact that Libet’s W precedes M is mentally consistent with W producing M. In one experiment, Wegner and Wheatley performed (13), they showed that subjects thought they caused an action, actually caused by someone else, by leading them to think about the action prior to its occurrence. The subject and an experimenter together manipulated a mouse that drove a cursor on a computer screen. The screen showed many objects. The object names were occasionally given in an auditory signal to the subject followed by the experimenter stopping the cursor on the named object. Subjects often had the sense that they had decided to stop the cursor on that object. Wegner has expanded on these ideas elsewhere (14).
NEUROLOGIC DISORDERS OF WILL
In neurology, there are many disorders in which the issue of will arises. There are patients who have movements that are commonly held as being involuntary. Myoclonus is such an example. The brain makes the movement, yet the patient interprets the movement as involuntary. Why should this be so? Chorea is another example. Yet, early in the course of their illness, patients with chorea often do not recognize that there are any involuntary movements. Why not? Are their brains interpreting everything that is done as voluntarily chosen at that time? Why does that change?
Although tics are generally considered involuntary, patients with tics often cannot say whether their movements are voluntary or involuntary. This may not be a relevant distinction in their minds. It is perhaps a better description to say that they can suppress their movements or they just let them happen. Tics look like voluntary movements in all respects from the point of view of EMG and kinesiology (15). Interestingly, they are often not preceded by a BP or only a brief BP (consistent with only an NS’ component), and hence the brain mechanisms for their production clearly differ from ordinary voluntary movement (16,17). The presence of a premovement potential was not correlated with the patient’s sense of voluntariness (17). The term “unvoluntary” has been suggested (18), but it is not clear how that helps us understand the physiology. If forced to choose voluntary or involuntary, patients will more commonly say that the movements were voluntarily performed.
Related posts:
 Freud and Psychogenic Movement Disorders
Psychogenic Dystonia and Reflex Sympathetic Dystrophy
Freud and Psychogenic Movement Disorders
Psychogenic Dystonia and Reflex Sympathetic Dystrophy
 Functional Paralysis and Sensory Disturbance
Treatment of Hypochondriasis and Psychogenic Movement Disorders: Focus on Cognitive-Behavioral Therapy
Functional Paralysis and Sensory Disturbance
Treatment of Hypochondriasis and Psychogenic Movement Disorders: Focus on Cognitive-Behavioral Therapy
 The Sodium Amytal and Benzodiazepine Interview and Its Possible Application in Psychogenic Movement Disorders
Treatment of Psychogenic Movement Disorder: Psychotropic Medications
The Sodium Amytal and Benzodiazepine Interview and Its Possible Application in Psychogenic Movement Disorders
Treatment of Psychogenic Movement Disorder: Psychotropic Medications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


