1 What is manic depression (bipolar disorder)?
1.2 What is bipolar affective disorder?
Psychiatrists may appear to be always changing the names of the illnesses that they treat but this is not always done just to confuse the innocent! Manic depression is a term that has been used for more than a century to cover psychiatric illnesses with the fundamental symptom of a mood change. Fifty years ago the term would have been used widely to cover not only those patients who had manic episodes but also to include those who only experienced severe depression. In the 1960s it became apparent that there are major differences between those patients that experience mania and those that only suffer from depression. The differences are particularly in the course and the family history of the two types of mood illness. However, the considerable overlap has always been recognised. In order to indicate the separation, two new terms were adopted: unipolar and bipolar–unipolar depression for those patients that only experience depression and bipolar affective disorder for those that experience mania (and usually also depression). It would make logical sense to also have a unipolar mania category but in fact the unipolar manics are so similar to the bipolars that this term has not been popular (see Q 1.13).
Manic depression is an unusual illness in that a number of people have a bipolar illness that is currently undiagnosed because so far they have only suffered from depression. Even though the illness might have started with depression in the teenage years it is only when mania appears in the twenties that the diagnosis can be made. The illness affects both genders in essentially the same way.
1.3 What do you call recurrent depression with hypomania?
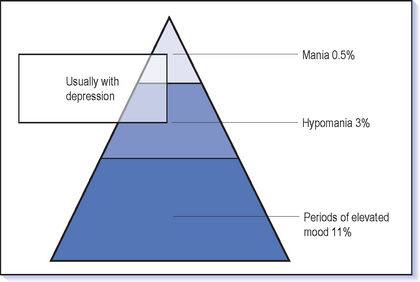
The dividing line between mania and hypomania is not easy to demarcate (see Q 1.7); however it is worthwhile making this distinction because it affects decisions about treatment (Fig. 1.1). For this reason a different name is given to depression with mania–bipolar I–in contrast to depression with hypomania–bipolar II. There have been attempts to define bipolar III and IV based on family history and the effect of antidepressants but these have not really caught on.
1.4 What are the symptoms of mania?
The following example of a manic woman illustrates the range of symptoms and behaviours characteristic of mania (see also Box 1.1).
 Mood: In order to make a diagnosis of mania there must be a change in mood. This is usually elevated and she feels elated, ‘great’, ‘fantastic’. Extreme terms are used to describe a state that few of us reach. She may well be feeling ‘better than ever’, and in an exciting and unique way ‘connected with the whole world’. It is common to have never had such a good feeling in the whole of her life. One of the major problems later can be that she doesn’t feel that this is an experience that she would like to avoid; in fact she feels just the opposite because it is a feeling that one would want to seek out. The closest comparison is to feelings that a great success or achievement (or winning the lottery) can produce or the high that comes from drugs such as cocaine. The elation is often infectious and others can (at first at least) feel more cheerful in her presence and find a smile on their face. She looks happy but in an active, excited way rather than displaying a calm peaceful serenity.
Mood: In order to make a diagnosis of mania there must be a change in mood. This is usually elevated and she feels elated, ‘great’, ‘fantastic’. Extreme terms are used to describe a state that few of us reach. She may well be feeling ‘better than ever’, and in an exciting and unique way ‘connected with the whole world’. It is common to have never had such a good feeling in the whole of her life. One of the major problems later can be that she doesn’t feel that this is an experience that she would like to avoid; in fact she feels just the opposite because it is a feeling that one would want to seek out. The closest comparison is to feelings that a great success or achievement (or winning the lottery) can produce or the high that comes from drugs such as cocaine. The elation is often infectious and others can (at first at least) feel more cheerful in her presence and find a smile on their face. She looks happy but in an active, excited way rather than displaying a calm peaceful serenity.BOX 1.1 The symptoms of mania
There must be a change in mood–elation or irritability–together with usually all of the following:








 Attention span: Attention can be intense but only for a short period. Concentration is poor because of distractibility, so that she cannot spend more than a few minutes on any task before setting off on another track. Memory is perceived to be good but may actually be poor because of the distraction and lack of focus. Afterwards she may have very poor recall of the events during the spell of mania.
Attention span: Attention can be intense but only for a short period. Concentration is poor because of distractibility, so that she cannot spend more than a few minutes on any task before setting off on another track. Memory is perceived to be good but may actually be poor because of the distraction and lack of focus. Afterwards she may have very poor recall of the events during the spell of mania.

 Speech: She will talk non-stop and be difficult to interrupt. Staying quiet becomes impossible and dialogue is not needed–monologue is fine. In fact she does not even need an audience: you can see her wandering about, chatting away. Talking may not be enough–singing, shouting and laughter all form part of expressing her joy to the world.
Speech: She will talk non-stop and be difficult to interrupt. Staying quiet becomes impossible and dialogue is not needed–monologue is fine. In fact she does not even need an audience: you can see her wandering about, chatting away. Talking may not be enough–singing, shouting and laughter all form part of expressing her joy to the world.Flight of ideas is the classic form of speech in mania (Box 1.2). Flight indicates the way ideas flow from one to another. The connections within the speech are usually apparent, in contrast to the thought disorder of schizophrenia which is much more obscure. But connections are too free and frequent so that distractions in what she sees or hears send her off on a new track. Alternatively, internal connections or personal memories may suddenly intervene. Playing with language is common as punning or rhyming takes over the flow for a while. The digressions mean that the goals of speech are quickly lost and so little is achieved in any conversation.
 Appetite: Appetite may be little changed though she will lose weight because essentials such as eating are not given much priority, or poor concentration and distractibility leave everything half eaten.
Appetite: Appetite may be little changed though she will lose weight because essentials such as eating are not given much priority, or poor concentration and distractibility leave everything half eaten. Disinhibition: You may notice the disinhibition from a distance with flamboyant, bright, eccentric clothes and a home visit reveals a spectacularly decorated house. It is always interesting to visit a house in the summer which is decked out for Christmas because ‘I’m the second coming’. However, be wary of the conservatively dressed Englishman whose dress belies his extraordinary behaviour.
Disinhibition: You may notice the disinhibition from a distance with flamboyant, bright, eccentric clothes and a home visit reveals a spectacularly decorated house. It is always interesting to visit a house in the summer which is decked out for Christmas because ‘I’m the second coming’. However, be wary of the conservatively dressed Englishman whose dress belies his extraordinary behaviour.
1.5 What psychotic symptoms accompany mania?
Paranoid ideas are the other type of delusion that is commonly seen in manic states. However, it can be difficult to tell when patients’ frustration with others’ lack of enthusiasm for their projects turns to paranoia. Paranoia always has a grandiose edge to it: ‘Why on earth would the CIA be interested in following you?’ Sometimes the mixture is more interesting–for example the man who has to leave the hospital as he is the only one who can tackle the drug traffickers who are in turn out to kill him. But remember paranoid ideas are common in a wide variety of psychiatric disorders (including confusional states) and are certainly not diagnostic of mania.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


