CHAPTER 11 Brief Psychotherapy: An Overview
Despite the notion that it is a long-term endeavor, most data indicate that psychotherapy as it is practiced in the real world has a short course. Therefore, it is usually “brief therapy” even if its duration is not specified as such at the outset. Well before the nationwide impact of managed care was felt, studies consistently showed that outpatient psychotherapy typically lasted 6 to 10 sessions. Data on national outpatient psychotherapy utilization obtained in 1987—early in the takeover of managed care—showed that 70% of psychotherapy users received 10 or fewer sessions. Only 15% of this large sample had 21 or more visits with their therapist.1
HISTORY OF BRIEF PSYCHOTHERAPY
The modern era started in the 1960s when Sifneos and Malan independently developed the first theoretically coherent, short-term psychotherapies. The increased activity of Ferenczi and Rank, Lindemann’s crisis work, Grinker and Spiegel’s push for brevity, Alexander and French’s flexible framework, and Balint’s finding and holding the focus were all technical innovations, but none constituted a whole new method. Malan and Sifneos each invented ways of working that were not a grab bag of techniques but each a whole new therapy, with a coherent body of theory out of which grew an organized, specified way of proceeding.2,3
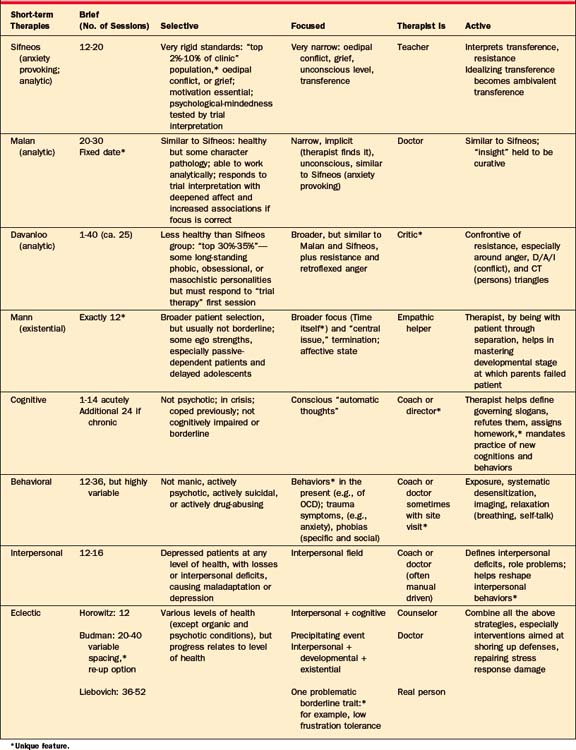
Over time, as therapies became briefer, they became more focused and the therapist became more active. But brevity, focus, and therapist activity are ways in which short-term therapies differ, not only from long-term therapy, but also typically from one another. Patient selection makes up a fourth “essence” in the description of the short-term psychotherapies. Table 11-1 shows brevity, selectivity, focus, and therapist activity as the organizing principles for the therapies summarized in the columns below each “essence.”
MODERN BRIEF PSYCHOTHERAPIES
There are four general schools of brief psychotherapy: (1) psychodynamic; (2) cognitive-behavioral; (3) interpersonal; and (4) eclectic. Each has indications and contraindications,4–6 but it is worth acknowledging at the outset that there is no conclusive evidence that any one short-term psychotherapy is more efficacious than another.7–10
Psychodynamic Short-term Therapies
Malan’s method11,12 is similar, but the therapist discerns and holds the focus without explicitly defining it for the patient. (In the initial trial, if the therapist has in mind the correct focus, there will be a deepening of affect and an increase in associations as the therapist tests it.) A unique feature of this treatment is that Malan sets a date to stop once the goal is in sight and the patient demonstrates capacity to work on his or her own. A fixed date (rather than the customary set number of sessions) avoids the chore of keeping track if acting out causes missed sessions or scheduling errors.
Malan’s work is reminiscent of the British object-relations school. Like Sifneos, he sees interpretation as curative, but he aims less at defenses than at the objects they relate to. In other words, the therapist will call attention to behavior toward the therapist, but rather than asking what affect is being warded off, Malan wants to know more about the original object in the nuclear conflict who set up the transference in the first place. Malan’s later work converges toward that of Davanloo’s,8,13,14 so that his and Malan’s approaches are conceptually similar.
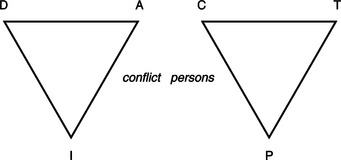
As shown in Figure 11-1, the therapist works with this “triangle of conflict”—which goes from defense (D) to affect (A) to impulse (I), in relation to the “triangle of persons.” This begins with a problematic current object (C), one mentioned in the first half of the initial interview. Then investigation moves to the therapist (T), who the patient has just been protecting from anger, and then to the parent (P) who taught such patterns in the first place. One or two circuits around the “D/A/I” (conflict) triangle in relation to three points of the “C/T/P” (persons) triangle constitute the “trial therapy.” This is a more elaborate version of the trial interpretations Malan and Sifneos use to test motivation and psychological-mindedness. Davanloo’s patients lack the ability to distinguish between points in the “conflict [Defense/Affect/Impulse] triangle” or to experience negative affects directly. By trolling the D/A/I triangle around the “persons [Current object/Therapist/Parent] triangle,” Davanloo forces the frigid patient to feel and creates a mastery experience for the patient.
The dynamic-existential method of James Mann15,16 relied on a strict limit of exactly 12 sessions. Time is not just a reality, a part of the framework, but time is an actual tool of treatment. Twelve sessions, which Mann chose somewhat arbitrarily, is sufficient time to do important work but short enough to put the patient under pressure. This set number with no reprieve is both enough time and too little. It thrusts the patient and the therapist up against the existential reality they both tend to deny: Time is running out.
No other short-term therapy seems to require so much of the therapist. And even if this method does not appeal to all short-term therapists, almost every subsequent theorist in the field seems to have been influenced by Mann to some degree—even Budman and Gurman,17 whose use of time appears so unlike Mann’s. It is described somewhat in detail here because the interaction of therapist activity with phases of treatment is so clearly highlighted.
Underlying the focus the patient brings, Mann posits a “central issue” (analogous to a core conflict) in relation to the all-important issue, “time itself.” The therapist is a timekeeper who existentially stays with the patient through separations, helping master the developmental stages in which parents failed the patient. Mann’s theoretical point of departure (which probably followed the empirical finding that 12 sessions was about right) is Winnicott’s18 notion that time sense is intimately connected to reality testing, a “capacity for concern,” and unimpaired object relationships. A better sense of time and its limits is the soil for growing a better sense of objects.
Cognitive-Behavioral Brief Therapies
The behavioral therapies have a decades-long history and a good record of achievement. The cognitive therapies are the inheritors of this earlier track record. What the two have in common is that neither addresses “root causes” of disorders of mental life, but focus almost exclusively on the patient’s outward manifestations. These “nonpsychological” or “non–insight-oriented” styles of therapy are broadly applicable, both in terms of patients and problems. (For the cognitive-behavioral therapies, see Chapter 16.)
The method of Aaron Beck19–21 aims at bringing the patient’s “automatic” (preconscious) thoughts into awareness and demonstrating how these thoughts affect behavior and feelings. The basic thrust is to challenge them consciously, and to practice new behaviors that change the picture of the world and the self in it. Beck says that an individual’s interpretation of events in the world is encapsulated in these fleeting thoughts, which are often cognitions at the fringes of consciousness. These “automatic thoughts” mediate between an event and the affective and behavioral response. The patient labors under a set of slogans that, by their labeling function, ossify the worldview and inhibit experimenting with new behaviors.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


