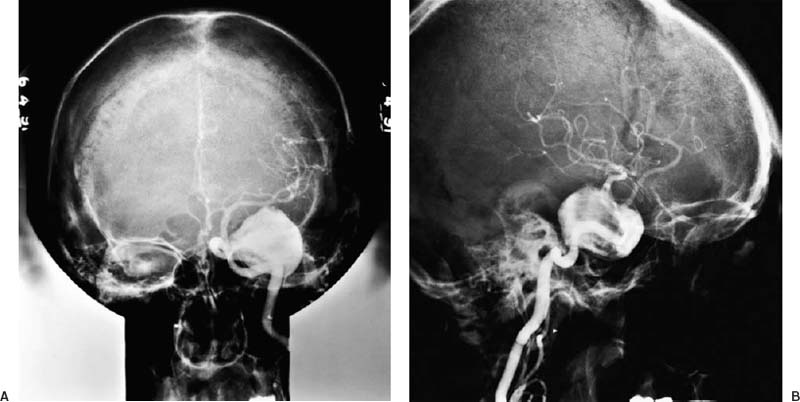
4 Diagnosis Giant aneurysm of the subclinoidal ICA Problems and Tactics This symptomatic giant aneurysm of the anterior genu region of the left internal carotid artery (ICA) was directly approached for direct repair or, if necessary, treatment with trapping and extracranial–intracranial (EC–IC) bypass. In the course of exposure of the aneurysm base, the aneurysm tore with broad disruption of the aneurysm neck. Temporary ICA trapping was performed, the aneurysm was resected off the parent artery, and the broad defect in the arterial wall was reconstructed with a venous patch graft. Keywords Giant cavernous ICA aneurysm, direct aneurysm repair, ICA reconstruction A 62-year-old woman presented with a progressive history over several months of left retroorbital pain, diplopia, and facial numbness and paresthesias. Examination revealed complete left sixth nerve palsy and partial third, fourth, and fifth (second division) nerve involvement. Magnetic resonance imaging (MRI) scan and left carotid angiogram had confirmed a giant (3.5 cm diameter) aneurysm of the “cavernous internal carotid artery” (Fig. 4–1). Before proceeding with treatment it was felt advisable to perform trial balloon occlusion (TBO) study and endovascular exploration of the aneurysm neck to define treatment strategies. Endovascular exploration of the aneurysm with a balloon catheter showed a broad aneurysm base off the lateral aspect of the ICA anterior genu, involving the C3 and distal C4 segment of the artery, which could not be occluded with a 10 mm balloon. Temporary balloon occlusion of the ICA was tolerated without symptoms. Baseline cerebral blood flow (CBF) was measured at 35 mL per 100 g per minute; with occlusion, the CBF dropped to 28 as measured by Xe131 washout. Based on the CBF measurements it was felt that the patient would be at increased risk for acute or delayed stroke with carotid sacrifice, and therefore planned treatment was exploration and clip reconstruction of the aneurysm neck or, if not possible, trapping of the aneurysm with collateral augmentation using EC–IC bypass. FIGURE 4–1 (A) Anteroposterior and (B) lateral left carotid angiograms demonstrating a giant intracavernous internal carotid artery aneurysm. Enhanced contrast at the anterior genu indicates the site of a broad aneurysm neck.
Giant Aneurysm of the Subclinoidal (Anterior Genu) ICA Treated with Aneurysm Resection and Reconstruction of ICA with Venous Patch
Clinical Presentation
Preoperative Evaluation
Surgical Procedure
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


