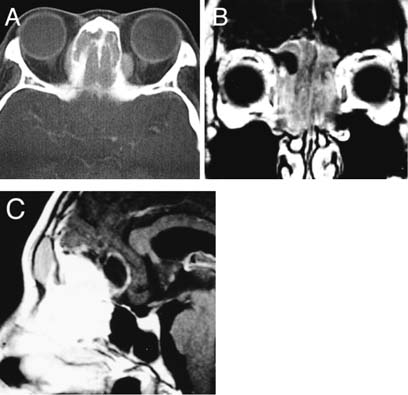
41 Diagnosis Olfactory neuroblastoma Problems and Tactics A 30-year-old woman suffered from olfactory neuroblastoma. The tumor occupied the nasal cavities and ethmoid sinuses, and invaded the orbits and frontal lobes. The lesion was removed en bloc with tumor-free margins. The defect was reconstructed with an inner table of the frontal bone and a free forearm flap anastomosed to the facial artery and vein. Malignant skull base tumors require craniofacial en bloc resection and simultaneous reconstruction by a multidisciplinary team consisting of neurosurgeons, otorhinolaryngologists, and plastic surgeons. Keywords En bloc resection, olfactory neuroblastoma, reconstruction, skull base A 30-year-old woman was referred to our institution with a 6-month history of anosmia. Computed tomography (CT) and magnetic resonance imaging (MRI) showed a mass in the anterior cranial base (Fig. 41–1). The tumor occupied the upper portion of the nasal cavities and the ethmoid sinuses, involved the nasal bone, and destroyed the medial orbital walls and the anterior cranial base. The tumor invaded into the orbits and the frontal lobes. Biopsy from the nasal cavity revealed that the tumor was olfactory neuroblastoma. A skull base surgery team consisting of neurosurgeons, otorhinolaryngologists, and plastic surgeons performed surgery. Through a coronal skin incision, a bifrontal craniotomy was performed. The dura was opened at the frontal base. The basal portion of the bilateral frontal lobes had tumor invasion and was separated from the normal brain. The arachnoid membrane and thin layer of the normal brain were left on the lesion as tumor-free margins. Then the dura was incised around the tumor on the planum sphenoidale and orbital roofs. Skull base osteotomies were made along the dural incision (Fig. 41–2). The orbital contents were separated from the medial orbital walls, where the periorbit was left on the lesion as a tumor-free margin. Facial osteotomies were made in the nasal bone and bilateral orbital floors (Fig. 41–2). The nasal septum and the mucosa were transected. Through the planum sphenoidale, a final osteotomy was made in the floor of the sphenoid sinus. The tumor was then removed in an en bloc fashion. Unfortunately in this patient, a small tumor mass was additionally removed from the right orbital floor. The dural defect was closed with a graft of the fascia lata. The medial orbital walls and the nasal bone were reconstructed using an inner table of the frontal bone. The defect in the anterior skull base and the reconstructed orbital walls and nasal bone were covered with a forearm flap anastomosed to the facial artery and vein (Fig. 41–3). The dura was tacked up and the free frontal bone was repositioned. FIGURE 41–1 (A) Enhanced computed tomography and (B,C) magnetic resonance imaging showing a mass in the anterior cranial base. The tumor occupies the nasal cavities and the ethmoid sinuses and invades the orbits and the frontal lobes. Postoperatively the patient had impaired ocular movement, which was recovered within 2 weeks. She received additional chemotherapy (cisplatin + etoposide) and 40 Gy focal irradiation. Two and half years later, tumor recurred in the right orbital roof. Surgical resections and radiation therapy were performed. At present, 5.5 years after initial surgery, she is alive with disease. Malignant tumors involving the skull base still pose a formidable surgical challenge. Although en bloc resection of malignant tumors with tumor-free margins is an established oncological principle
Olfactory Neuroblastoma with Brain Invasion
Clinical Presentation
Surgical Technique
Outcome
Key Points
Related posts:
 3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
50 A Large Petroclival Meningioma with a Fibrous Capsule
4 Giant Aneurysm of the Subclinoidal (Anterior Genu) ICA Treated with Aneurysm Resection and Reconstruction of ICA with Venous Patch
3 Surgical Management of a Challenging Giant Paraclinoid Aneurysm
38 Total Removal of a Recurrent Craniopharyngioma
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
6 Giant Internal Carotid Artery–Superior Hypophyseal Artery Aneurysm
50 A Large Petroclival Meningioma with a Fibrous Capsule
4 Giant Aneurysm of the Subclinoidal (Anterior Genu) ICA Treated with Aneurysm Resection and Reconstruction of ICA with Venous Patch
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


