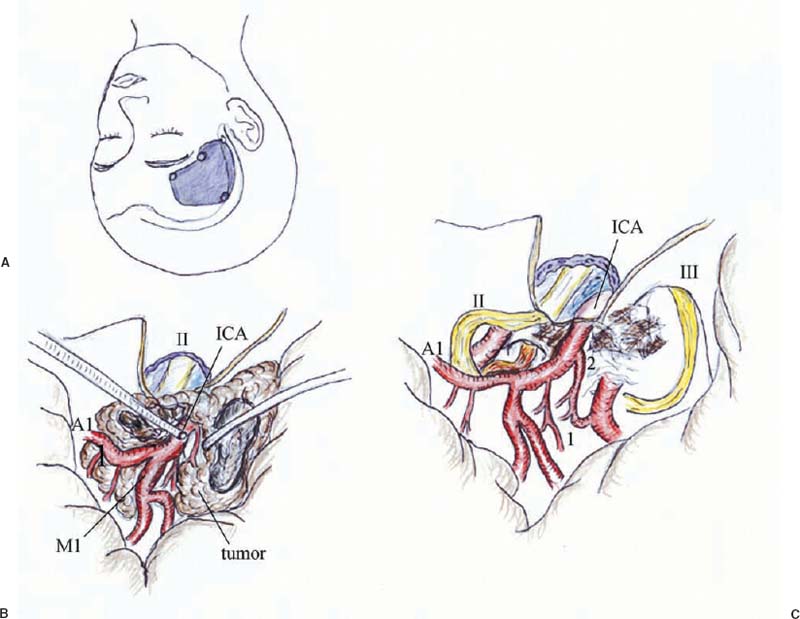
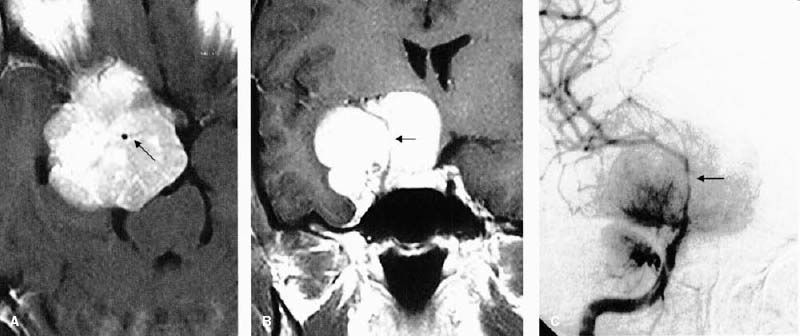
45 Diagnosis Meningioma arising from the anterior clinoid Problems and Tactics A huge, highly vascular anterior clinoidal meningioma encasing the internal carotid artery was found in a woman with progressive visual deficits. We used a skull base technique and were able to preserve the internal carotid artery (ICA). Keywords Clinoidal meningioma, internal carotid artery, perforators, optic nerve, skull base technique This 31-year-old woman developed right visual disturbance 6 months before admission. She was pregnant and almost full term. Her vision on the right was limited to counting fingers in front of her face. Magnetic resonance imaging (MRI) showed a huge mass in the right parasellar region (Fig. 45–1A,B). The internal carotid artery (ICA) was located in the center of the enhanced mass, indicating that the tumor had completely encased the ICA. Carotid angiograms showed a highly vascular tumor and narrowing of the ICA (Fig. 45–1C). The patient tolerated the balloon occlusion test of the right ICA. After undergoing Cesarean section she was referred to us for surgical treatment of the tumor. The patient’s head was turned 45 degrees to the left and fixed with a three-pin head rest. She was appropriately prepared and draped not only in the scalp area but also in the areas of the neck and right thigh in anticipation of a possible high-flow bypass in case of accidental or intentional ICA sacrifice in the course of tumor removal. Then right frontotemporal craniotomy was performed (Fig. 45–2). Before opening the dura, the sphenoid wing was extensively drilled away, the optic canal was un-roofed, and the anterior clinoid process was removed. The dura was incised and the sylvian fissure was widely opened to expose the meningioma. Although the tumor was very large, it was soft; therefore, its lateral part was removed in piecemeal fashion using ultrasonic aspiration and tumor forceps. The branches of the middle cerebral arteries were followed proximally to expose the main trunk (M1) and the ICA. Bleeding from the tumor was moderate and well controlled with a bipolar coagulator. After confirming the location of the ICA, the attachments of the tumor to the dura around the ICA dural ring were separated using a bipolar coagulator. The ICA and its branches, the anterior choroidal arteries and the posterior communicating arteries, were completely embedded within the tumor (Fig. 45–2). Because the arachnoid membrane was preserved in the cleavage between the tumor and the cerebral vessels, however, tumor separation from the arteries was relatively easy. The ICA was narrow due to compression by the surrounding tumor, but the arterial wall seemed to be free of tumor invasion. Although the right optic nerve was markedly displaced by the tumor in a superomedial direction, it was well preserved (Fig. 45–2). The tumor was totally resected with preservation of all important arteries and nerves. The dura at the site of tumor attachment was coagulated sufficiently. There was no invasion of the tumor into the cavernous sinus. The dural defect around the optic canal was repaired using fascia from the temporal muscle. FIGURE 45–1 (A,B) Preoperative enhanced magnetic resonance imaging and (C) right carotid angiogram showing a huge vascular tumor with complete encasement of the internal carotid artery (ICA) (arrow). Note narrowing of the ICA.
Clinoidal Meningioma Encasing the Internal Carotid Artery
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


