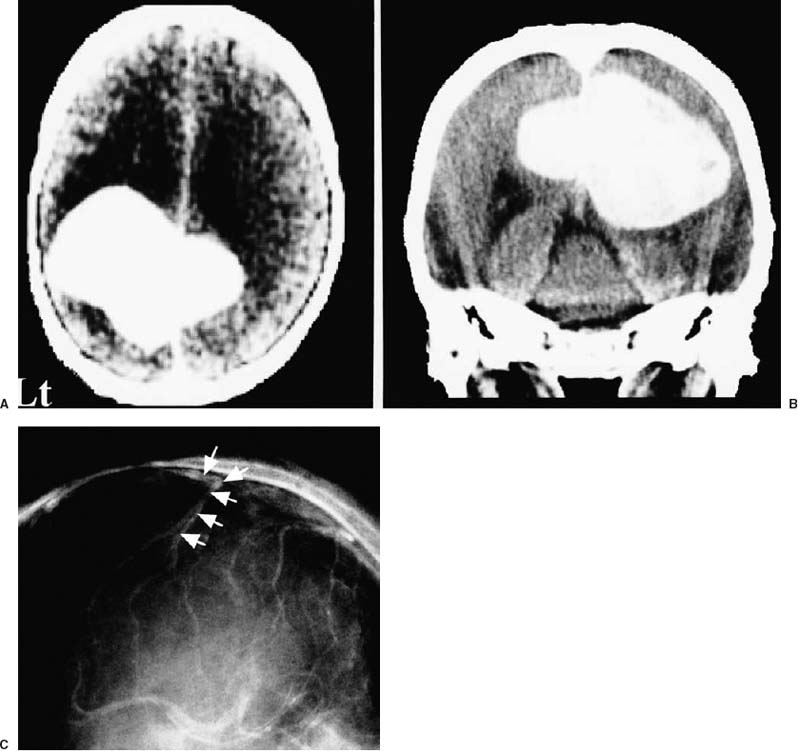
47 Diagnosis Falx meningioma Problems and Tactics The huge, dumbbell-shaped falx meningioma (9 × 8 × 6 cm) was located at the interhemispheric portion of the bilateral parietal region in the bilateral parietal lobe. It was totally removed by performing end-to-end anastomosis of the superficial cortical vein, which intercepted the approach to the tumor. Keywords Giant meningioma, vein anastomosis, falx meningioma, bridging vein, end-to-end anastomosis A 70-year-old woman presenting with right hemiparesis, right hemianopsia, and memory disturbance was found to have a huge, dumbbell-shaped falx meningioma that primarily extended into the left parietal lobe (Fig. 47–1A,B). The superficial cortical vein emptying into the superior sagittal sinus lay in the left parietal lobe (Fig. 47–1C). With the patient in the semisitting position and the neck slightly flexed, bilateral parietal craniotomy was performed. The middle meningeal arteries were coagulated with bipolar forceps to stop the blood supply to the tumor. After opening the dura of the left parietal area, the superficial cortical vein draining into the superior sagittal sinus was visualized. It intercepted the interhemispheric approach route (Fig. 47–2A). First, the vein was dissected and mobilized; however, this did not provide sufficient working space for the surgical procedure. We decided to cut the vein temporarily and anastomose it after removal of the tumor. Temporary clips were placed on the vein (Fig. 47–2B), which was cut 25 mm lateral from the superior sagittal sinus (Fig. 47–2C). This facilitated the approach to the tumor. The left portion of the tumor was resected piecemeal and the right portion was removed from the left side via the transfalcine approach.1 Following total removal of the tumor, the vein was stitched together by end-to-end anastomosis using 10–0 monofilament nylon and interrupted sutures (Fig. 47–2D). The caliber of the vein was 1.2 mm. The temporary clips were then removed, thus restoring the venous blood flow. The anastomosed site was confirmed to be patent. The time from cutting the vein to restoration of the venous blood flow after vein anastomosis was ~7 hours. During and after the surgical procedure, slight brain swelling and petechiae on the brain surface were noted. FIGURE 47–1 Computed tomographic images, (A) coronal and (B) axial, demonstrating a falx meningioma with bilateral extension. (C) Left carotid angiogram, lateral view and venous phase, showing the ascending parietal cortical vein (arrows). The vein intercepted the interhemispheric approach to the tumor. Postoperatively, the patient manifested no clinical signs of venous infarction or neurological deficits. A computed tomographic scan showed no signs of infarction or brain edema (Fig. 47–3A). She was discharged 1 month after the operation with no neurological deficits. A cerebral angiogram obtained 3 months postoperatively reconfirmed the patency of the vein (Fig. 47–3B).
Huge Falx Meningioma Removed by Using End-to-End Anastomosis of the Superficial Cortical Vein for Obtaining a Wide Operative Field
Clinical Presentation
Surgical Technique
Outcome
Key Points
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


