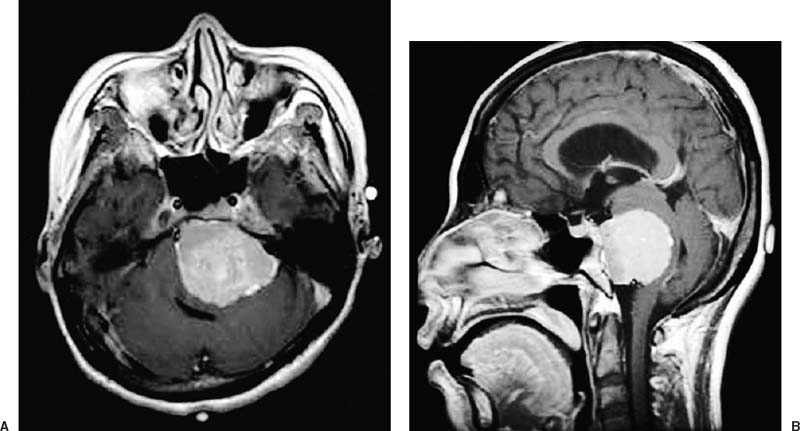
48 Diagnosis Petroclival meningioma Problems and Tactics A large petroclival tumor compressed the brain stem and resulted in multiple cranial nerve palsies and cerebellar dysfunction in a young, otherwise healthy woman. To achieve maximal cytoreduction and to prevent postoperative neurological deterioration, surgical resection using a combined skull base approach was undergone. Keywords Petroclival meningioma, transtentorial approach, retrolabyrinthine transsigmoid approach A 36-year-old woman presented with a 1-year history of tinnitus and a 5-month history of unsteady gait. Neurological examination revealed hypesthesia of the left trigeminal nerve, nystagmus, lower cranial dysfunction, cerebellar dysfunction, and left lower extremity weakness. Magnetic resonance imaging (MRI) showed a 5 × 5 × 4.5 cm mass in the left petroclival region that markedly compressed the brain stem and cerebellum (Fig. 48–1A,B). The patient was positioned supine with the head turned parallel to the floor, inclined slightly downward to minimize torsion to the contralateral jugular vein, and fixed to the operating table with the Mayfield head holder. Spinal drainage, which would aid exposure and be crucial in preventing postoperative cerebrospinal fluid (CSF) leakage, was prepared. The retroauricular C-shaped incision was used in a gentle curving fashion around the ear to expose the lateral temporal bone, external auditory meatus, and mastoid and suboccipital region. A subtemporal and suboccipital craniotomy was performed in one piece to expose the transverse and sigmoid sinuses (TS and SS) simultaneously. The otologist performed the approach through the temporal bone. A high-speed drill system was used for the mastoidectomy portion of the procedure. To preserve hearing and according to anatomic extension of the mass (Fig. 48–1A,B) a retrolabyrinthine approach was performed. The posterior and superior semicircular canals were skeletonized by drilling as far anteriorly as possible, both above and below the otic capsule, to expose as much dura as possible. The bone was removed over the superior petrosal sinus (SPS) and the SS. As a result, an intraoperative view showed the exposed SPS, SS, and jugular bulb with the dura intact. The endolymphatic sac and duct were preserved. Monitoring of electroencephalography, somatosensory evoked potentials, and facial and other cranial nerves was undertaken. The dura was incised over the temporal lobe at the anterior limit of the craniotomy (Fig. 48–2A). The incision was extended posteriorly to at least 1 cm below where the SPS enters the SS. Care should be exercised to avoid injuring a low-lying vein of Labbé that is attached to the temporal dura or tentorium. After coagulation of the SPS the tentorial margin adherent to it was transected anteriorly toward the petrous apex. The tentorium was also transected in a lateromedial direction fashioning a triangularly shaped tentorial flap with its curved base medially toward the incisura and its apex laterally toward the petrous ridge (Fig. 48–2A). In the edge of the incisura the fourth cranial nerve was verified. To ligate the SS, test clamping using a Yasargil temporary clip was done for 80 minutes. There was no evident brain swelling, and the ligation of the SS was then done (Fig. 48–2A). The temporal lobe and the cut tentorium were protected by retractors that allowed the base of the temporal lobe to be elevated without stretching the vein of Labbé. This maneuver with retraction of the cerebellum exposed the main mass. The mass extended to the tentorium and displaced the lower cranial nerves. Internal debulking using a surgical aspirator was done easily and dissection between the mass and brain stem was done uneventfully. Ipsilateral fourth, sixth, and seventh–eighth nerve complex and the lower cranial nerves were verified and separated successfully. The basilar artery, posterior cerebral artery, ipsilateral posterior communicating artery, and optic nerve were also identified and preserved (Fig. 48–2B). Gross-total removal was done successfully and meticulous bleeding control and irrigation were done. The temporal and occipital dura was reapproximated and artificial dura was used for the small defect. Abdominal adipose tissue, temporalis muscle, and fibrin glue were used to obliterate the temporal bone defect. The skin was closed layer by layer and spinal drainage of CSF was done for 5 days.
Meningioma of the Petrous and Clival Region
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


