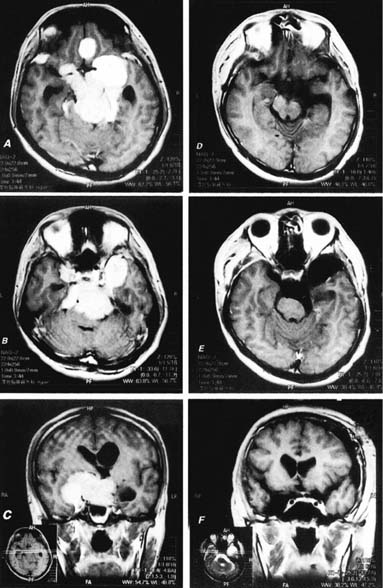
49 Diagnosis Bilateral megasize petroclival meningioma Problems and Tactics An extremely large petroclival meningioma originating from the left side and extending to the bilateral skull base area was detected on magnetic resonance imaging (MRI) due to progressing symptoms of quadriparesis and ataxia. Because of the huge size of the mass with severe compression to the brain stem in an otherwise healthy young man, urgent surgical intervention was indicated. There was no indication for any type of radiation therapy. This case demonstrates one of the largest petroclival meningiomas in the author’s personal series of 240 cases during the past 20 years. The tumor was engulfing the bilateral intradural carotid arteries and multiple bilateral cranial nerves, and also involved the bilateral cavernous sinus. Keywords Skull base meningioma, petroclival tumor, cavernous sinus, cranial nerves The patient was a 22-year-old man who had just graduated from a university and was looking for a job when he gradually noted mental slowness, headache, bilateral blurry vision, dysarthria, progressing quadriparesis, and ataxia. These symptoms were gradually becoming prominent and severe during the 6-month period preceding the patient’s visit to the Atsuchi Neurosurgical Clinic for neurological evaluation. The examination revealed significant ataxia, imbalance, moderate quadriparesis, and dysarthria. Subsequent enhanced magnetic resonance imaging (MRI) revealed a giant-size petroclival meningioma extending bilaterally and also elevating the brain base and compressing the brain stem (Fig. 49–1A–C). Because of the progressing ataxia, quadriparesis, and blurry vision, urgent neurosurgical management was indicated. This patient’s general physical condition was otherwise normal without any pulmonary, abdominal, or cardiovascular diseases. We considered three operative approaches to this tumor; namely, a left frontotemporal transcavernous approach,1 an extended middle fossa anterior petrosectomy approach,2 and a combined transpetrosal approach.3,4 Because of the patient’s bilateral blurry vision, We made it a priority to separate and decompress the bilateral optic nerve and chiasm; therefore, the left orbitocranial and frontotemporal transcavernous approach was selected for the initial surgical approach. The first surgical intervention was performed on December 18, 2000. The patient was placed in a supine position with the head supported with a three-pin skull clamp. The head was rotated to the right 45 degrees and moderately hyperex-tended to provide easy access to the clinoidal and optic nerve area. A standard left frontotemporal craniotomy was performed. The extradural dissection was advanced along the orbital roof, sphenoid ridge, and lateral orbital wall. The orbitocranial skull base was shaved flat in a maximum way using the Anspach power diamond drill (Anspach Companies, Palm Beach Gardens, FL) with automatic irrigation system. The sphenoid ridge was drilled totally away to expose the meningoorbital band, which was incised ~7 mm. The optic canal unroofing was performed with continuous irrigation, and the anterior clinoid process of the left side was then removed carefully with 2-mm and 3-mm coarse diamond burrs. The superior orbital fissure was then exposed and We confirmed the foramen rotundum. The standard pericavernous extradural temporopolar dissection6 was completed and the entire epidural area was cleaned up for hemostasis. FIGURE 49–1 (A–C) Preoperative enhanced magnetic resonance imaging (MRI) of the megasize bilateral petroclival meningioma. (D–F) Final postoperative enhanced MRI showing radical total resection of this extensive skull base meningioma.
Radical Total Resection of a Giant Petroclival Meningioma
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


