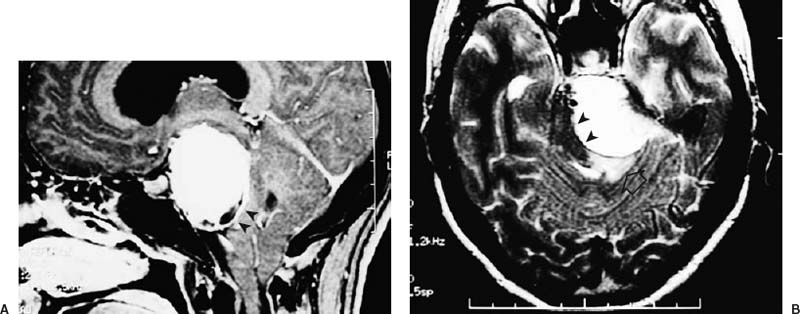
50 Diagnosis Meningoliomatous meningioma in the petroclival region Problems and Tactics A petroclival meningioma demonstrated an enhanced capsule on magnetic resonance imaging (MRI) and showed more severe adhesion to the engulfed cerebral arteries than expected before surgery. Subcapsular enucleation of the tumor was important to avoid significant surgical complications, and the surgeon has to know the signs from MRI. Keywords Petroclival meningioma, surgical technique, tumor capsule, adhesiveness This 35-year-old-female, a pediatric doctor, complained of headache and left facial paresthesia. She had no cerebellar sign of long tract signs, nor other cranial nerve deficit, except for the trigeminal nerve. Her hearing was normal on both sides. Magnetic resonance imaging (MRI) showed a left petroclival meningioma of 45 mm in diameter (Fig. 50–1). The posterior margin was 20 mm higher than the posterior clinoid process. The tumor margin was smooth with a capsular enhancement between the brain stem. On T2 image a small, high-intensity area was demonstrated in the cerebellopontine angle (CPA), where a limited adhesion was suspected; however we suspected that most of the tumor margin would be dissectable except for the CPA because the patient symptoms were mild and the tumor margin was smooth. The patient was operated on by the left anterior transpetrosal approach. She was placed in the supine-lateral position. A left ventricular drainage tube was placed to reduce retraction on the temporal lobe. A left temporal craniotomy was made above the external auditory meatus and root of the zygoma. The middle fossa dura was dissected from the base, preserving the greater superficial petrosal nerve (GSPN). The middle meningeal artery was coagulated and cut, and the pyramisal apex was exposed. The pyramidal apex was resected as much as possible while preserving auditory structures. The superior petrosal sinus was ligated above the IAM and cut with the tentorium. The posterior fossa side of the tentorium was covered with meningioma, which was dissected from each leaflet of the tentorium. On the posterior margin of the tumor, the seventh and eighth cranial nerves were comfirmed to be adherent to the consistent and fibrous tumor capsule. The tentorial artery, a main tumor feeder, was coagulated during tumor dissection from the anterior leaflet of the tentorium. The trochlear nerve and the superior cerebellar artery were engulfed and adherent to the upper margin of the tumor. The trigeminal nerve was atrophic and deviated inferomedially, which suggested the tumor capsule was considerably adherent to the basilar system; it was found that complete removal including the capsule was impossible. Therefore, intracapsular tumor removal was done, and a portion (a few millimeters thick) of the capsule was not dissected from the brain stem (Fig. 50–2). Confirmation of the thickness of the capsule was suspected from pulsation and bulging of the capsule. FIGURE 50–1 (A) A sagittal section of gadolinium-enhanced magnetic resonance imaging (gd-MRI) showing a meningioma with a thick capsule (arrowheads) in the petroclival region. The tumor extends superiorly, 20 mm higher than the posterior clinoid process. (B) An MRI T2 image demonstrates the tumor and compressed brain stem (arrowheads). The basilar artery (arrow) attaches on the tumor, and perifocal edema is seen in the cerebellopontine angle (open arrow).
A Large Petroclival Meningioma with a Fibrous Capsule
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


