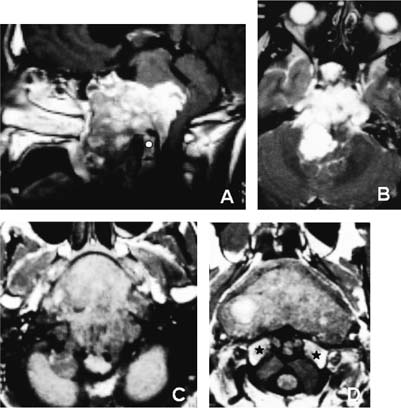
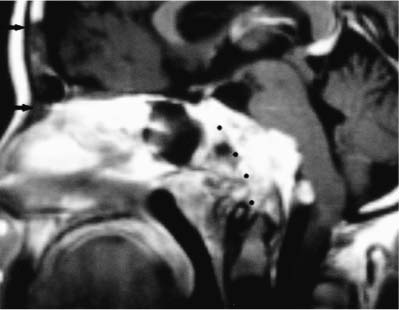
54 Diagnosis Extensive intra-extradural chordoma of the whole clivus Problems and Tactics A huge chordoma involving the whole clivus and extending into the intradural space was discovered in a heathly young man. The strategy included three surgical stages to achieve as radical a resection as possible and to stabilize the craniocervical junction. The treatment was completed with proton therapy. The patient is in very good neurological condition and disease free at 4 years. Keywords Chordoma, clival tumor, skull base, tumoral approach This 19-year-old man had complained for 2.5 years of nasal obstruction and breathing difficulties. Despite imaging studies discovering a clival tumor, he refused any surgery for 2 years until the tumor growth led him to accept a surgical treatment. He also presented a transient left sixth cranial nerve palsy. The computed tomographic (CT) scan and magnetic resonance imaging (MRI) showed a huge heterogeneous tumor involving the whole clivus extending ante-riorly toward the cavum, inferiorly to the C1 and C2 vertebrae, and posteriorly into the posterior fossa through the dura (Fig. 54–1). Comparing the imaging studies at 2 years’ delay, a significant tumoral growth could be demonstrated. The first step consisted of debulking the preclival part of the tumor through a transbasal approach. The patient was in the supine position with the head straight and slightly extended. A small bifrontal bone flap was created with the inferior cutting passing through the orbital ridge and the frontonasal suture. The dura of the anterior fossa was then elevated with sacrifice of the olfactory nerves. The bone of the anterior fossa was resected on the midline down to the jugum sphenoidalis. The tumor was discovered extending into the sphenoidal sinus and removed down to the C2 level. Anteriorly the posterior part of the nasal septum and nasal mucosae were resected. Lower the mucosae of the cavum was kept intact and the tumor behind it was resected up to the anterior arch of the atlas. Above C1 a layer of tumor was left in front of the dural plane (Fig. 54–2). The dura was not opened at any place even at the level of the olfactory nerves because they were cut very low. Nevertheless, a pericranium graft was sutured to the dura of the anterior fossa to reinforce the dura (Fig. 54–2). The second step involved resection of the tumor extending through the dura through a transoral–transpalatal approach. Closure with a free forearm graft pediculated on the facial vessels. Ten days later a transoral–transpalatal approach was performed after lumbar drainage and a tracheostomy had been placed; the palate was cut circumferentially, following the teeth and 5 mm medial to them, and kept pediculated on the mucosa on one side. For this the mucosa was cut on the midline of the uvula and then laterally along the palate on one side. The mucosa and the muscular layers were cut on the midline of the cavum. The exposure then started on the inferior part of the tumor at the level of C2 with drilling of the anterior arch of C1 and of the odontoïd process. Starting from a normal dura, the tumor was then resected using curettes and the ultrasonic aspirator. The remaining pieces of bone of the clivus were resected beyond the tumoral limit. The occipital condyles were totally resected on the left side and partially on the right. The left twelfth cranial nerve was divided intradurally. The intradural tumoral extension was progressively extirpated. The dura was widely resected beyond the tumoral infiltration. At the end of the tumor re-section the two vertebral arteries, the basilar trunk, and all the cranial nerves from XII to VI could be seen. FIGURE 54–1 Preoperative MRI. (A) Saggital view. Notice the intradural and pharyngeal extension. White circle indicates the odontoïd process. (B–D) Axial view. Notice the intradural extension and in (D) the tumoral development in front and behind the occipital condyles (black stars). FIGURE 54–2
Extensive Intra-extradural Chordoma of the Whole Clivus
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


