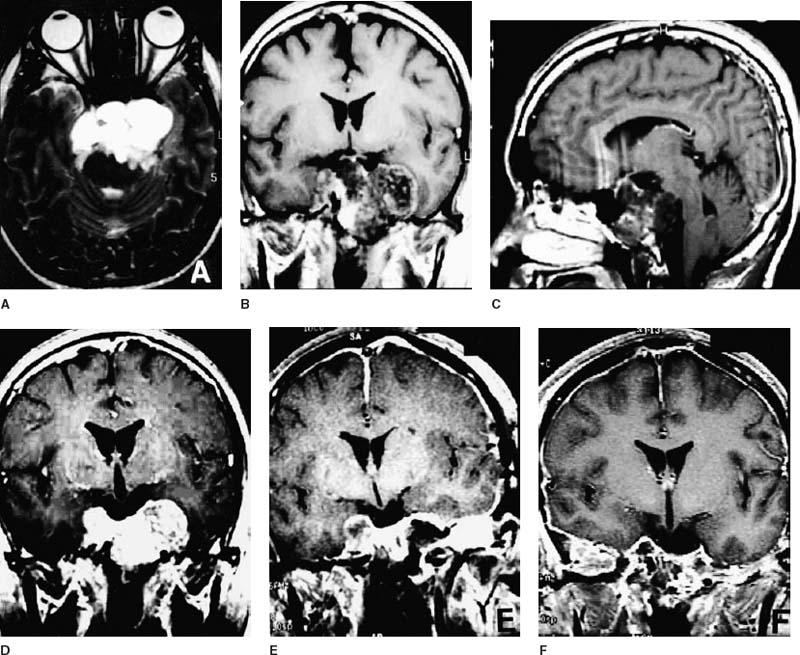
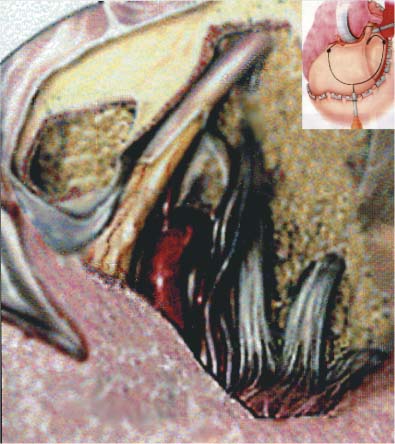
56 Diagnosis Bilateral cavernous sinus extension of a chordoma Problems and Tactics We present the case of a residual skull-base chordoma invading both cavernous sinuses in a young man who underwent partial surgical resection of the tumor at another institution. Despite the risks presented by an additional surgery in the skull base, radical removal of such a tumor is possible and should be the goal to control the disease better before the patient undergoes radiation therapy. Keywords Chordoma, skull-base tumor, surgical approach, tumor excision A 30-year-old man came to us for evaluation 2 months after undergoing surgical resection of a clival chordoma at another institution. Before the first surgery, he reported having a 2-year history of diplopia in his left lateral gaze and a 2-month history of numbness and paresthesias in the territory of innervation of the second and third trigeminal branches. Magnetic resonance imaging (MRI) revealed a large mass involving the clivus and both cavernous sinuses. The tumor extended into the posterior fossa, compressed the brain stem, eroded the left petrous apex, and extended through the left petroclival junction into the left lateral and posterior nasopharynx (Figs. 56–1A–C). The patient underwent a midface de-gloving approach, which was complicated by postoperative meningitis that was treated successfully. After surgery, his facial paresthesias partially resolved, but he continued to have diplopia. This first surgery removed the medial portion of the mass from the petroclival junction and the mid- and lower thirds of the clivus to the dorsum sella, decompressing the brain stem, but the lobular extensions into both cavernous sinuses and middle cranial fossae persisted (Fig. 56–1D). An assessment of the patient for proton beam therapy recommended having the remainder of the tumor resected. The patient was then referred to us for resection of the residual tumor in these critical areas. We performed two procedures separated by an 8-day interval. The first procedure was a left cranioorbital zygomatic approach (COZ) (Fig. 56–2) including a petrous apicectomy and resection of the middle fossa floor. The patient’s head was placed in the Mayfield headrest and turned 45 degrees to the right. The frameless stereotactic fiducials were registered. Monitoring devices were positioned for cranial nerves III, V, VII, and X and brain stem auditory potentials and somatosensory evoked potentials. A frontotemporal incision was extended from the midline to curve behind the hairline to just in front of the tragus. The superficial temporal artery and the pericranium were preserved. The frontal branch of the facial nerve was dissected in a subfascial manner. The pericranium was divided near the vertex and was reflected downward in a single flap with the temporalis muscle. A single cranioorbital flap and the rest of the orbital roof were removed. Sectioning the anterior root of the zygoma and removing the roof of the glenoid fossa allowed us to create a single flap and further reflect the temporalis muscle inferiorly. Under the microscope, the dura of the middle fossa was elevated with sharp dissection to prevent injury to the greater superficial petrosal nerve. The middle meningeal artery was coagulated and divided as it emerged from the foramen spinosum. After the superior orbital fissure was exposed through resection of the sphenoid wing, the floor of the middle fossa was resected by drilling out the anteromedial (between V1 and V2) and the anterolateral (between V2 and V3) triangles. FIGURE 56–1 Initial magnetic resonance imaging (MRI). (A) coronal, (B) axial, and (C) sagittal views demonstrating chordoma extension into the cavernous sinus bilaterally. (D) Coronal MRI after resection using the anterior approach with residual tumor in both cavernous sinuses. (E) Coronal MRI after tumor resection using the cranioorbital zygomatic approach, with residual tumor in the right cavernous sinus. (F) Coronal MRI after the right zygomatic middle fossa approach achieving gross tumor resection. The tumor was found medial to the pterygoid plate after the anterolateral triangle was drilled. The petrous apex was drilled posterior to the third division of the trigeminal nerve and anterior to the cochlea all the way out to the clivus. The outer layer of the cavernous sinus was relaxed and the temporal lobe was elevated without traction on V2 or V3. The bulk of the tumor was identified and resected beneath the roots of the trigeminal nerve along the petrous apex. The sphenoid sinus was entered by further drilling of the anteromedial triangle, and the previous fat graft was identified as free of tumor. The tumor medial to the pterygoid plate, between V2 and V3, was removed. The carotid artery was identified posterior to V3 after significant debulking of the tumor. The tumor superior, medial, and inferior to the carotid was cleaned out and no lateral extension was seen. The inner layer of the lateral cavernous sinus between V2 and V3 was entered and the superior portion of the tumor was resected. The clivus beneath the trigeminal nerve was drilled out all the way to the contralateral side, and the medial aspect of the right cavernous sinus and the intracavernous carotid artery were identified. Tumor in the contralateral cavernous sinus was lateral to the cavernous carotid and could not be removed from the left-side approach. In the posterior fossa, an intradural extension of the tumor that did not breach the arachnoid plane was identified and removed. An abdominal fat graft and fibrin glue were used to cover the defects left by drilling and tumor removal. Vascularized tissue from the posterior limb of the temporalis muscle was placed along the middle fossa and extended medially into the cavernous sinus to the contralateral petrous apex. Closure proceeded in the ordinary fashion. FIGURE 56–2
Chordoma
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


