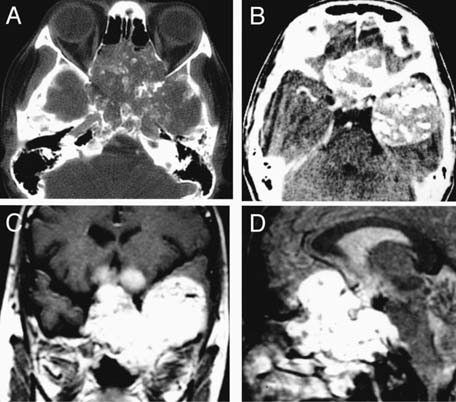
57 Diagnosis Huge chondrosarcoma Problems and Tactics A huge mass in the skull base was found in a 36-year-old woman with Maffucci’s syndrome. The tumor occupied the nasal and paranasal cavities and extended to the anterior, middle, and posterior intracranial spaces. The midline skull base structures and the left middle cranial base were destroyed. Surgical resection was planned because she presented with decreased right visual acuity and left papilledema. Epidural skull base approach (combined anterior craniofacial and orbitozygomatic approach) was selected to remove the tumor and a bipedicled temporoparietal galeal flap with vascularized outer table graft was utilized to reconstruct the large skull base defect. Keywords Anterior craniofacial approach, chondrosarcoma, galeal flap, orbitozygomatic approach, skull base A 36-year-old woman with Maffucci’s syndrome was referred to our institution with decreased vision (8/20) and optic disc atrophy in the right eye and papilledema on the left. Plain computed tomography (CT) showed a mass in the anterior and middle cranial bases with calcifications of various sizes. The sphenoid and ethmoid sinuses, the medial wall of the left orbit, and the anterior and middle cranial bases were destroyed by the tumor. Enhanced magnetic resonance imaging (MRI) showed intracranial tumor extension through destroyed clivus and anterior and middle cranial bases. Both sides of the orbital apex and optic canal, the sella turcica, and the left side of the cavernous sinus, the nasal cavity, and the maxillary sinus also were involved (Fig. 57–1). Angiography showed displacement of the left carotid artery without tumor stain. The patient tolerated the balloon occlusion test of the left internal carotid artery for 15 minutes. A skull-base surgery team consisting of neurosurgeons, otorhinolaryngologists, and plastic surgeons performed surgery. A coronal skin incision was made. Subfollicular dissection was used to preserve the temporoparietal galea. A bifrontal and left temporal craniotomy was then performed (Fig. 57–2A), and an orbital bar including the orbital roofs, the nasal bone, and the left zygomatic arch was removed (Fig. 57–2B). After circumferential osteotomy around the cribriform plate, the nasal mucosa and septum were transected 1 cm below the cribriform plate. The affected left lateral orbital wall, middle cranial base, and pterygoid plate were removed via the left orbitozygomatic route. The foramen rotundum and the maxillary nerve were involved, and the mandibular nerve and the cavernous sinus were compressed by the tumor. The left superior orbital fissure, optic canal, and carotid canal were released from lesioned bone. The tumor and the affected sella floor, the upper two thirds of the clivus, and the medial bony walls of the left and right cavernous sinuses were removed via the anterior craniofacial approach. The right optic canal was released. The tumor was located mainly in the epidural space. There was a small dural hole at the destroyed clivus through which the tumor penetrated. The invaded nasal septum, nasal mucosa, and left middle concha were removed. The tumor under the left eye and in the left maxillary sinus was removed using an endoscope. Finally, the entire gross tumor mass was completely removed (Fig. 57–2C,D). FIGURE 57–1 (A) Plain and (B) enhanced computed tomography showing a mass in the anterior and middle cranial bases with calcifications of various sizes. (C) Gadolinium-enhanced coronal and (D) T2-weighted sagittal magnetic resonance imaging demonstrates that the tumor occupies the paranasal and nasal cavities and extends to the anterior, middle, and posterior intracranial spaces.
Huge Chondrosarcoma in the Skull Base
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
19 Partially Thrombosed Giant Dissecting Aneurysm of the Vertebral Artery—Treatment Strategies
 18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
18 Combined Endovascular and Surgical Treatment of a Large Basilar Trunk Aneurysm in a Child
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


