76 Acquired Myopathies
Clinical Vignette
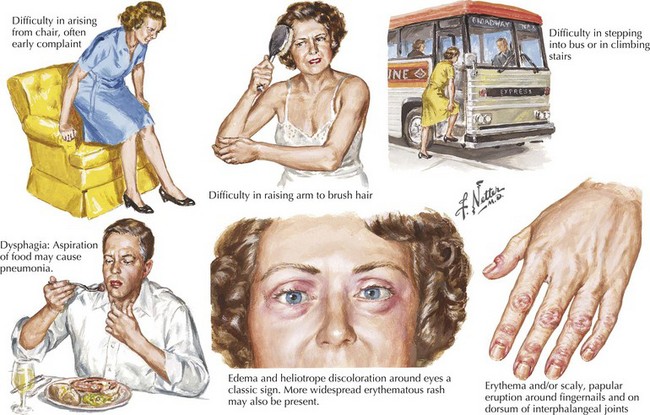
The common nongenetically determined myopathies are classified into those having a primary inflammatory process, an underlying endocrinopathy, a toxic pathophysiology, or an underlying associated systemic disorder. Much less commonly, a few infectious agents, such as trichinosis, may lead to a primary myopathy. Myopathies typically present with symmetric symptoms and signs of muscle weakness affecting the proximal limbs and paraspinal musculature (Fig. 76-1). Asymmetric, distal, generalized, or regional patterns of weakness also occur in certain distinct myopathies such as inclusion body myositis (IBM). Less commonly, ventilatory muscles or cardiac muscles are primarily affected. Myopathies occasionally present with periodic weakness, exercise-induced muscle pain, or stiffness.
Diagnostic Approach
Laboratory Evaluation
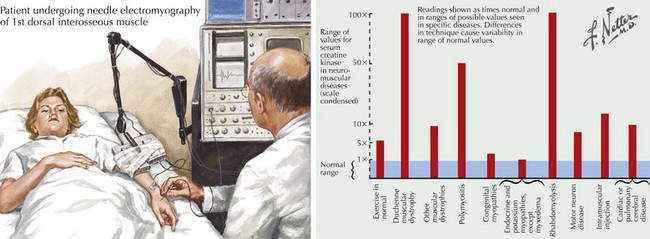
The serum CK is characteristically increased in many myopathies; this may vary from a 2- to 50-fold increase, although in most myopathies CKs are usually in the 500–5000 IU/mL range (Fig. 76-2). When this enzyme is abnormally elevated, its serum levels do not closely parallel disease severity or activity. Serum aldolase levels are also frequently elevated in myopathies; its increase generally parallels the increase in CK, although many clinical neuromuscular specialists do not routinely order an aldolase level. However on occasion it may be elevated with a normal CK as illustrated in the Cushing syndrome vignette reported later in this chapter.
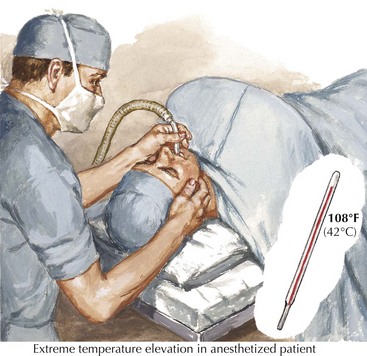
Patients with persistently increased CK levels sometimes associated with muscle pain but without clinically demonstrable weakness, family history, or exposure to potentially myotoxic substances are classified as having hyperCKemia. Despite thorough clinical and laboratory examination, it is often difficult to assign a specific pathophysiologic mechanism to this finding. HyperCKemia is often an elusive clinical challenge. However, it is important to emphasize that although no diagnosis per se is defined, the finding of hyperCKemia deserves serious consideration. Such individuals are at an increased risk of developing malignant hyperthermia (MH) if they require surgery under general anesthesia. Certain induction agents, particularly the halogenated ones, namely halothane, are particularly prone to inducing this life-threatening complication in patients with hyperCKemia. Therefore, we suggest that our hyperCKemia patients wear a MedAlert bracelet to always call the attention of anesthesiologists to this finding and thus potentially prevent an episode of MH (Fig. 76-3).
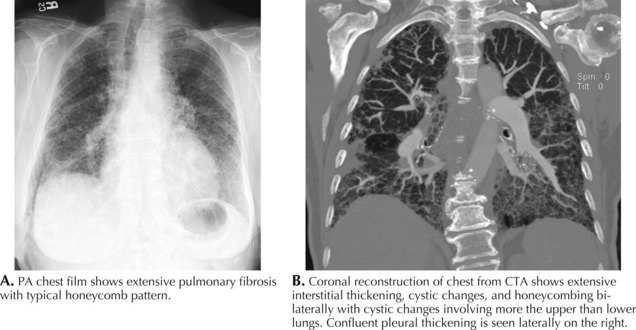
The serum myositis-specific and myositis-associated antibodies are other testing parameters that are useful in the evaluation of some patients with a myopathy. However, as these are present in fewer than half of all patients with polymyositis and dermatomyositis, routine serologic testing for these antibodies is of limited use. The presence of anti-Jo-1 (antibody to histidyl t-RNA synthetase) antibodies suggests potential end organ comorbidity, for example, interstitial lung disease (Fig. 76-4). Signal recognition particle antibodies are most often associated with necrotizing myopathies and may suggest a poor treatment response.
Electromyography
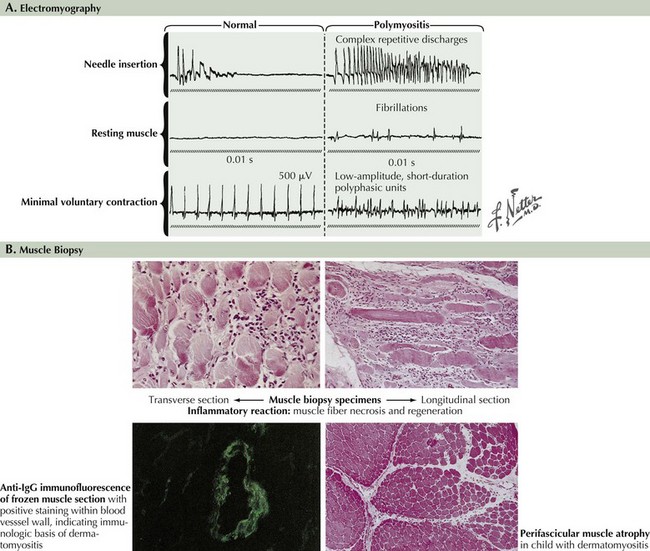
EMG evaluation of patients with suspected myopathies is important (Fig. 76-5, and see Fig. 76-2). Results of routine nerve conduction studies are normal in myopathies, with the exception of diminished compound muscle action potential amplitudes in more severe disorders. The primary EMG abnormalities in the myopathies are classically found at the time of the needle examination. Classic findings of a myopathy include the presence of abnormally low amplitude, short duration, and polyphasic motor unit potentials (MUPs). It is typical for these patients to have both an early recruitment and increased numbers of MUPs early on in the muscle activation for a given effort. Destruction of myofibrils or muscle membrane results in abnormal insertional activity, particularly fibrillation potentials and complex repetitive discharges. Inflammatory myopathies, several dystrophies, and various myotonic muscle disorders may be distinguished by the presence of myotonic potentials on needle EMG.
Muscle Biopsy
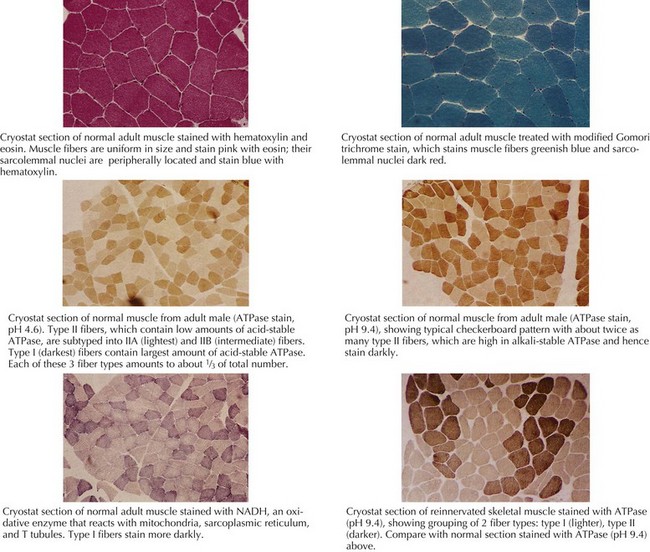
Muscle biopsy is the definitive diagnostic tool for many myopathies (Fig. 76-6). The selection of the biopsy site is important; muscles that are unaffected, that are severely affected (are at end stage), or have been recently subjected to EMG evaluation should be avoided. Muscles commonly biopsied include the vastus lateralis, deltoid, and biceps brachii. The gastrocnemius muscle is often avoided due to the possibility of incidentally discovered neurogenic atrophy. The upper lumbosacral muscles, thoracic paraspinal muscles, such as the multifidus, and much less commonly the cervical paraspinal muscles provide an alternative site for biopsy. On reflection one recognizes that these muscles are indeed the most proximal ones and thus more prone to show early changes of an active myopathic process.
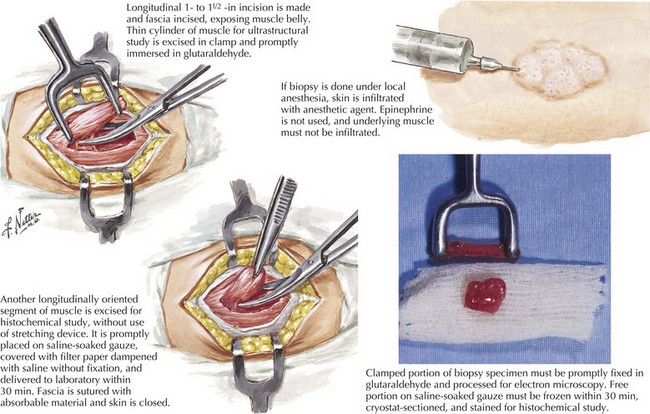
The muscle biopsy specimen per se is divided into separate aliquots for formalin fixation, paraffin embedding, and immediate freezing. The formalin-fixed piece is stained with hematoxylin and eosin (H and E) because this permits a rapid means for initial evaluation. This is especially useful for identifying inflammatory myopathies where such a diagnosis offers the potential for successful therapeutic intervention. Frozen specimens are best for other stains, including nicotinamide adenosine dinucleotide dehydrogenase (NADH), modified Gomori trichrome, adenosine triphosphatase, and lipid and glycogen stains (Fig. 76-7 and see Fig. 76-5).