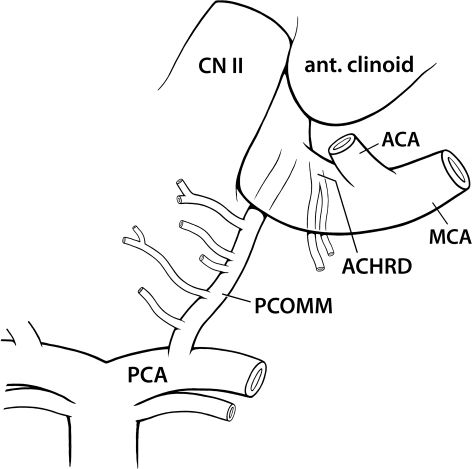
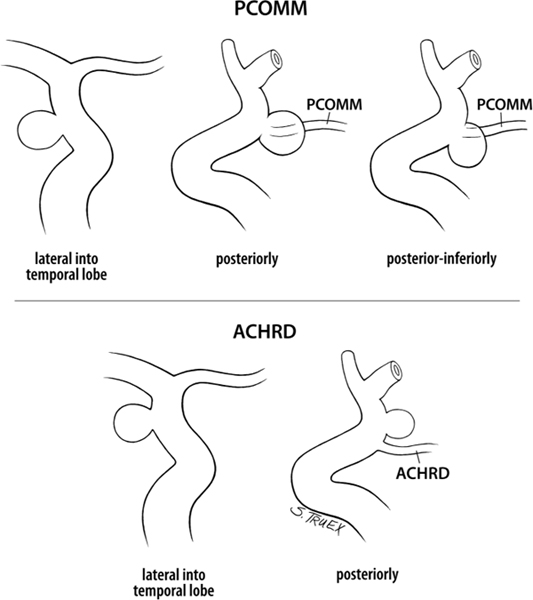
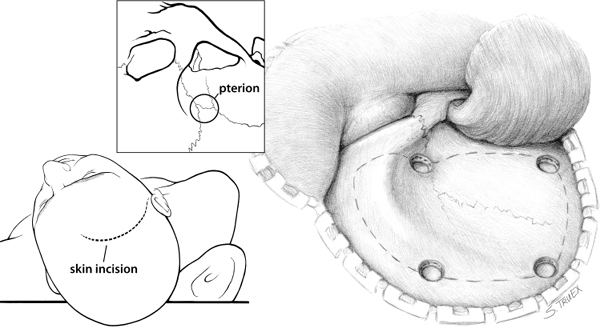
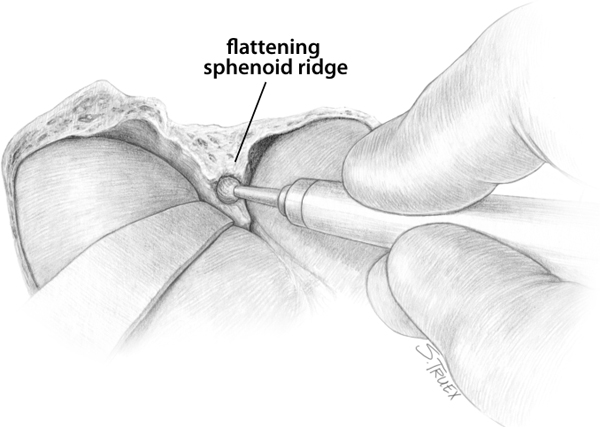
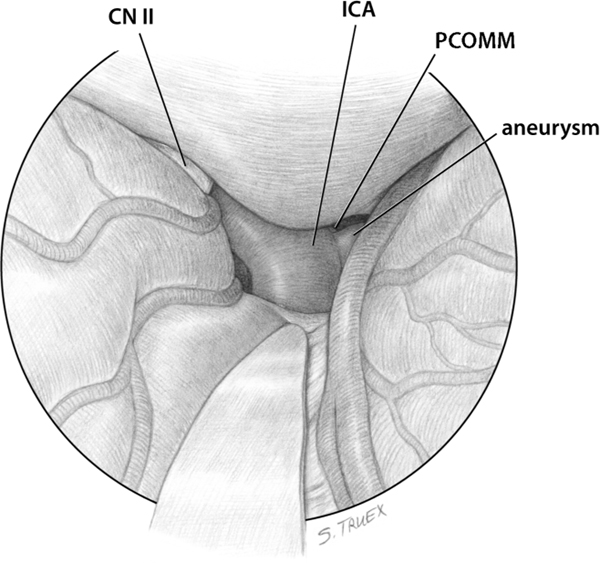
3 Following anterior communicating artery aneurysms, internal carotid artery–posterior communicating artery (ICA-PCOMM) aneurysms are the most common causes of aneurysmal subarachnoid hemorrhage, and these two sites taken together account for fully a third of all intradural, intracranial aneurysms. Although aneurysms in these locations are generally felt to be among the easier vascular surgical challenges, there are unique features of each of these aneurysms that can significantly impact both the technical difficulty of their management and the outcome of their surgical treatment. Because of the relative frequency of these lesions, we’ll use their discussion to briefly describe our standard version of the frontotemporal or “pterional” craniotomy, used throughout this book for the treatment of aneurysms of the carotid and distal basilar circulations. The PCOMM varies in size from trivial to being as large as the posterior cerebral artery in 15 to 20% of individuals. It originates from the posterior aspect of the ICA 2–4 mm distal to the anterior clinoid process (Fig. 3.1), is directed medi-ally in its posterior course to penetrate the membrane of Liliequist, and terminates in the posterior cerebral vessel some 3 to 4 mm lateral to the basilar apex. Its only branches are four to eight anterior thalamoperforating arteries, which emerge from its superior aspect and pass through the roof of the interpeduncular fossa en route to the anterior thalamus and lateral basal ganglia. Fig. 3.1 Anatomy of the posterior communicating artery. The anterior choroidal artery (ACHRD) is uniformly a much smaller artery, rarely greater than 1 mm in diameter. It arises millimeters distal, and slightly lateral, to the posterior communicating vessel from the posterior-lateral aspect of the ICA proximal to the bifurcation. Often double or more frequently bifurcating immediately after its origin, the ACHRD uniformly provides an early branch to the mesial temporal lobe (the uncal artery) then passes superiorly and medially around the mesial temporal lobe to enter the choroidal fissure and then the temporal horn of the lateral ventricle. Its terminal branches supply varying areas of the internal capsule, limbic system, and basal ganglia. The ACHRD’s small size, intimate approximation to the deep aspect of the carotid, and important parenchymal distribution make it a frequent source of morbidity in surgical procedures involving the carotid cistern and anterior temporal lobe. Aneurysms of the posterior aspect of the carotid wall project either laterally (Fig. 3.2) into the temporal lobe (both PCOMM and ACHRD), posteriorly (both PCOMM and ACHRD), or posterior-inferiorly (uniquely PCOMM). The direction of projection is not only important in terms of the classic hemorrhage pattern, but also influences the operative approach to each lesion. The aneurysms that project laterally or posteriorly are usually unassociated with the third cranial nerve: however, those that project inferiorly or inferolaterally routinely are in direct contact with the nerve itself along its medial border. Especially long “windsock” aneurysms may actually extend beneath the oculomotor nerve, elevating it and deviating it laterally. Fig. 3.2 Aneurysms of the posterior carotid wall. Optimal position of the patient’s head encourages the brain to drop away from the inner table of the skull and decreases the amount of brain retraction necessary to visualize the area of interest. In operations directed at the posterior carotid wall, the major impediments to exposure are the orbital cortex of the frontal lobe and the temporal tip. Hyperextension of the neck maximizes the degree of frontal lobe displacement by gravity, but the head should only be rotated away from the operative side the minimal amount necessary to permit exposure of the posterior carotid wall without requiring mandatory retraction of the temporal lobe. In general, this is ~30 degrees. However, if there are mitigating factors which suggest that more exposure of the posterior aspect of the carotid cistern would be advantageous (very large aneurysm, extensive neck, temporal lobe clot, multiple aneurysms, etc.) we suggest rotating the head fully 45 degrees away from the operative side and mobilizing the temporal tip posteriorly with a second retractor blade, as demonstrated in the management of distal basilar artery aneurysms. These aneurysms are routinely operated via one of many variations of a lateral subfrontal, frontotemporal, or transsylvian exposure. A small (4 × 5 cm) fronto-temporal craniotomy, centered on or about the pterion, is combined with a generous subtemporal craniectomy of the squamosal temporal bone and a subsequent aggressive extradural removal of the bony sphenoid wing (Figs. 3.3 and 3.4). The inner table of the intact frontal calvarium is removed to facilitate exposure of the anterior aspect of the sylvian fissure, and then the dura is opened low along the entire length of bony defect and tacked back against the inner table. It’s possible to expose both ICA-PCOMM and ICA-ACHRD aneurysms via an exclusive subfrontal approach by simply elevating the posterior aspect of the orbital cortex, opening the carotid cistern and then dissecting along the posterior carotid wall until the aneurysm or parent vessel is encountered. The limited visualization provided by this “sneak and peek” exposure (Fig. 3.5) is generally adequate for clip ligation of small posteriorly and laterally projecting aneurysms of both posterior communicating and anterior choroidal origins, providing intraoperative hemorrhage doesn’t occur and assuming preservation of the parent arteries is not a high surgical priority. Fig. 3.3 Skin incision and frontotemporal craniotomy. Fig. 3.4 Extradural flattening of sphenoid ridge. Fig. 3.5 Initial surgical view of internal carotid artery. The initial step in a somewhat more conservative approach involves a variable opening of the horizontal segment of the sylvian fissure. When dealing with a tense, edematous, postsubarachnoid hemorrhage brain, especially with a laterally projecting aneurysm, a wide opening of the fissure from the middle cerebral bifurcation to the carotid cistern is advisable. This provides the maximum transsylvian and subfrontal exposure while simultaneously decreasing traction on the temporal lobe and attached aneurysm. After the institution of ventricular drainage and completion of a wide opening of the fissure, very frequently no temporal lobe retraction is necessary once the frontal lobe retractor has been placed on the orbital cortex at the level of the carotid bifurcation. If the brain isn’t “hot” or there is significant cerebral atrophy, opening only the medial several millimeters of arachnoid covering of the fissure may be adequate to provide ample visualization of the entire length of the carotid artery, again without significant posterior retraction of the temporal tip. This can be accomplished by first gently elevating the orbital cortex while inspecting the arachnoid reflection over the horizontal segment of the fissure. Approximately half the distance from the lateral cortex to the basal cisterns, the arachnoid is opened superficially, and then the exposure is deepened gradually with sharp dissection as the retractor blade is advanced medially across the posterior aspect of the orbital cortex (Fig. 3.6).
Aneurysms of the Internal Carotid Artery at the Origins of the Posterior Communicating and Anterior Choroidal Arteries
General
Anatomy
Projection
Procedure
Positioning
Craniotomy
Initial Approach
Related posts:
 The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Vertebral Artery at the Origin of the Posterior-Inferior Cerebellar Artery
Aneurysms of the Proximal Internal Carotid Artery
The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Vertebral Artery at the Origin of the Posterior-Inferior Cerebellar Artery
Aneurysms of the Proximal Internal Carotid Artery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


