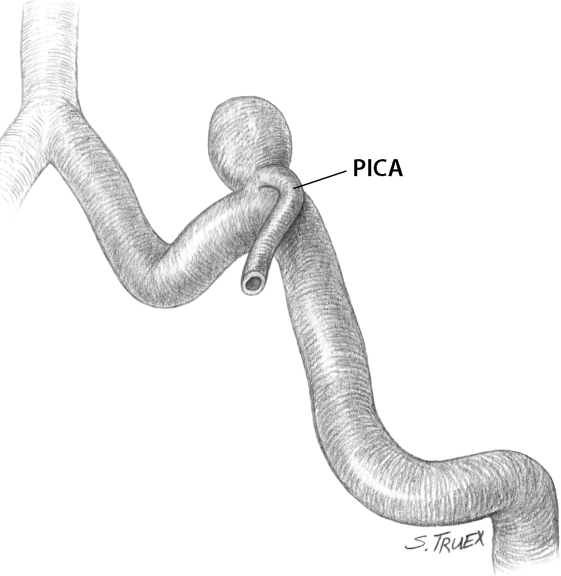
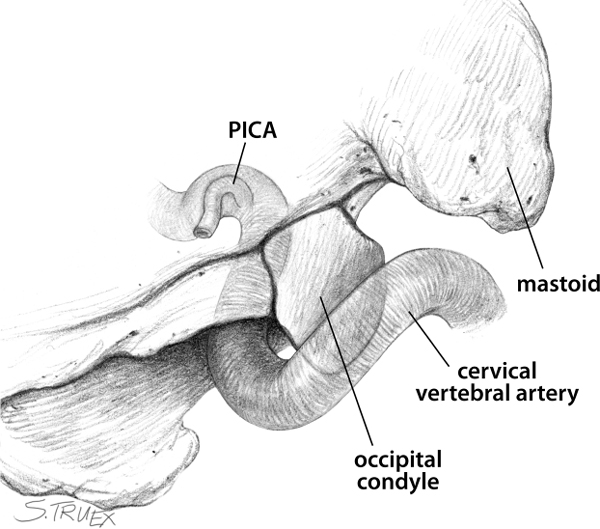
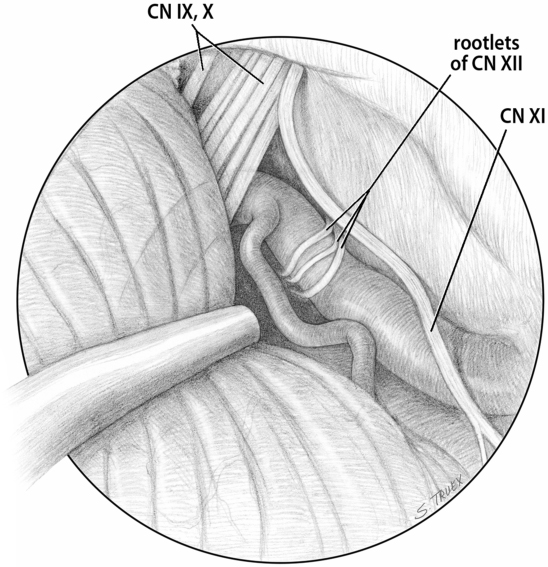
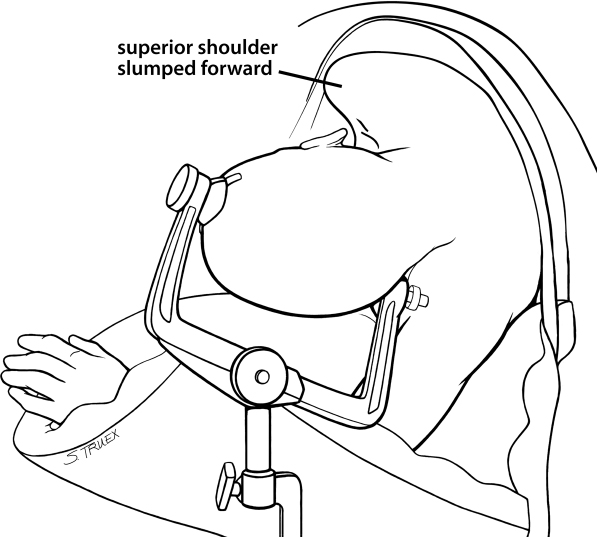
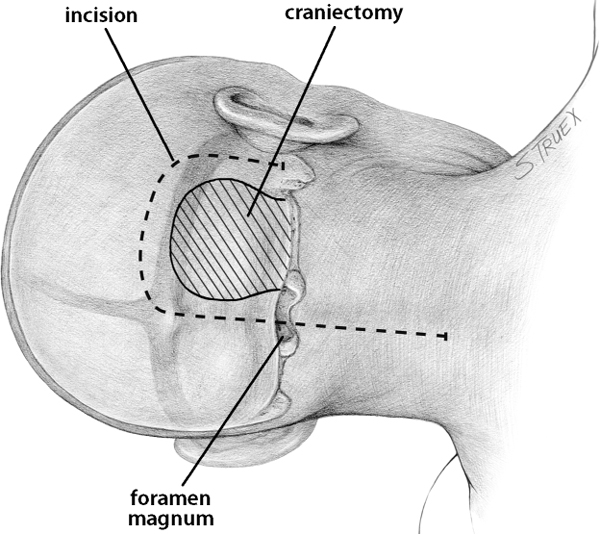
9 Vertebral artery (VA) aneurysms represent the second most common aneurysm site in the posterior circulation and are the only vascular lesions (aside from vascular cranial nerve compression) commonly occurring in the cerebellopontine angle (CP angle). These aneurysms may originate from the vertebral artery proximal to the posterior-inferior cerebellar artery (PICA) origin, or from the VA distal to the PICA, but the vast majority occur in association with the PICA origin. The PICA, which often shares a reciprocal size relationship with the anterior-inferior cerebellar artery, routinely takes origin from the VA just after it enters the cranial cavity via a short dural tunnel, and aneurysms may arise at any branch point along its course; the second most common site of PICA aneurysms is the posterior medullary segment at the angiographic choroidal point. A constant characteristic of VA-PICA aneurysms is their tendency to incorporate a significant length of the initial portion of the PICA in the aneurysm neck. The short segment of the intracranial VA proximal to the PICA origin is generally directed superiorly, but as the PICA emerges, the parent artery bends medi-ally toward the midline and its ultimate junction with the contralateral VA (Fig. 9.1). Awareness of this change in trajectory becomes important when the surgeon seeks to establish essential distal control of the VA, for as a rule the artery must be identified and isolated medial to the aneurysm-bearing segment, not rostral along the lateral aspect of the medulla. Fig. 9.1 Common orientation of PICA aneurysms. Although cervical PICA origins are not uncommon, both novice and experienced surgeons often find themselves surprised by the very proximal location of the routine intracranial VA-PICA origin (Fig. 9.2). This point is generally found in the inferior aspect of the cerebellopontine angle almost exactly at the rostral-caudal level of the jugular tubercle; the intracranial length of the VA from its exit from the dural tunnel to the PICA origin is generally quite short and is shrouded from view from below by the overhanging posterior lip of the occipital condyle. This shallow intracranial location puts a surgical premium on aggressive exposure of the craniocervical junction prior to dural opening, both for adequate exposure of the aneurysm-bearing segment of artery and for the establishment of proximal arterial control. The intracranial VA is overlain laterally by the ascending spinal root of the spinal accessory nerve (CN XI) and encircled medially against the stem by the emerging rootlets of the hypoglossal (CN XII), which almost always are found immediately proximal to the PICA origin (Fig. 9.3). Slightly more distally, the rootlets of the glossopharyngeal (CN IX) and vagus (CN X) nerves lie suspended superficial to the PICA and the VA in a wide arachnoid sheath that funnels them to the internal jugular foramen. Immediately superficial to these rootlets, the choroid plexus is invariably seen peeking through the foramen of Luschka. In the rare situation in which a retractor is required for exposure of these aneurysms, it should be placed gently on the cerebellar flocculus at this level. Fig. 9.2 Common bony association of VA-PICA origin. Fig. 9.3 Association of cranial nerve XII and PICA. VA-PICA aneurysms generally project in a rostral direction to some extent; however, their critical axis of projection is either posteriorly into the medulla itself or anteriorly into the subarachnoid space of the CP angle cistern. Very frequently, the previously described medial bend of the VA, when coupled with the aneurysm’s projection, will strongly influence the optimal route of surgical exposure of the VA distal to the aneurysm neck. These patients are operated in the lateral, “park bench” position with the operative side superior (Fig. 9.4). The neck is fully flexed in the “military brace” position and the vertex inclined toward the floor slightly. The superior shoulder is allowed to slump, and then is drawn and fixed with wide tape anterior to the coronal plane of the body. Each of these maneuvers maximizes the surgeon’s access to the lateral subocciput. Patients with VA-PICA aneurysms are operated in the lateral decubitus position (aneurysm side up) via an exposure popularized by Roberto Heros that has come to be known as the suboccipital, far lateral approach (Fig. 9.5). This is a difficult exposure to learn, but one that greatly facilitates all exposures of the cerebellopontine angle. Do all the steps correctly and your patients will prosper. In our version of this procedure, the key steps are as follows: 1. Vigorous reflection of the suboccipital muscle bulk inferiorly 2. A generous suboccipital craniectomy that includes the posterior and lateral aspects of the foramen magnum 3. A limited removal of the posterior-medial aspect of the occipital condyle 4. Removal of the ipsilateral lamina of the first cervical vertebra 5. Opening of the dura so as to maximize lateral exposure Fig. 9.4 Lateral position for the suboccipital, far lateral approach. Fig. 9.5 Skin incision and craniotomy for suboccipital, far lateral approach. While this procedure can be done via an S-shaped or even a linear incision, we believe a hockey stick or shepherd’s crook incision offers the best superficial exposure to the cervical musculature. This incision extends superiorly from the mastoid tip to the inferior nuchal line, then medially to the midline and finally inferiorly to the midcervical area. The skin, subcutaneous tissue, and superficial layer of suboccipital muscles are reflected laterally and inferiorly to be held there with fishhook retractors (Fig. 9.6). The surgeon then palpates the insertion of the inferior oblique and the origin of the superior oblique muscles at the lateral mass of C1, and sections those with the monopolar cautery (Fig. 9.7). With careful dissection, both the superficial and the deep suboccipital musculature can then be elevated from lateral to medial while cutting the muscles’ attachment to the subocciput, leaving a fascial cuff superiorly. When the midline is reached, the incision proceeds inferiorly to disconnect the muscular attachments to the arch of C1 and lamina of C2. The entire muscle cuff is then reflected inferiorly below the lamina of C1 to be held by spring-loaded retractors under tension.
Aneurysms of the Vertebral Artery at the Origin of the Posterior-Inferior Cerebellar Artery
General
Anatomy
Projection
Procedure
Positioning
Craniotomy and Initial Approach
Reflection of Suboccipital Muscles
Related posts:
 The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Internal Carotid Artery at the Origins of the Posterior Communicating and Anterior Choroidal Arteries
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Proximal Internal Carotid Artery
The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Internal Carotid Artery at the Origins of the Posterior Communicating and Anterior Choroidal Arteries
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Proximal Internal Carotid Artery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


