Chapter 27 Anterior Approaches to the Lumbar Spine
RETROPERITONEAL APPROACH WITH A PARAMEDIAN INCISION
INCISION
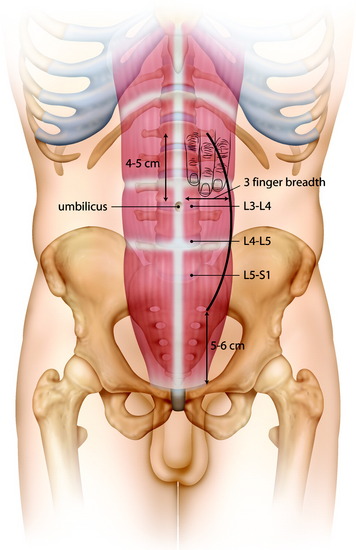
The incision starts from 4–5 cm superior to the umbilicus, and reaches to 5–6 cm superior to the pubic symphysis (Fig. 27-1).
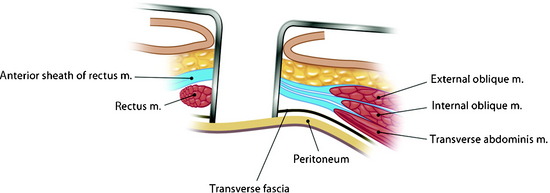
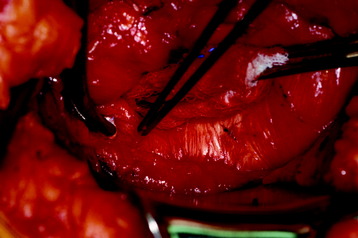
RECTUS MUSCLE INCISION
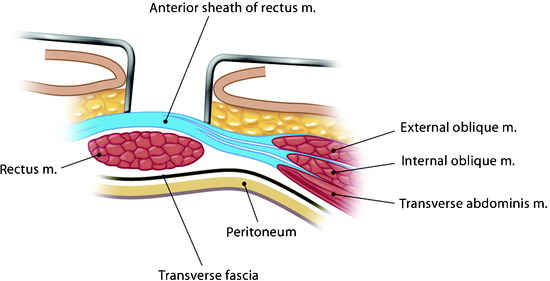
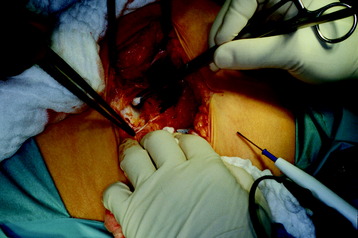
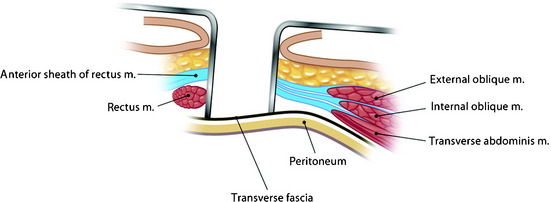
The anterior rectus sheath is incised (Figs. 27-2 and 27-3). During the incision, superficial epigastric vessels may be encountered and sacrificed. The rectus muscle is mobilized and retracted medially to expose the posterior sheath (Figs. 27-4 and 27-5). The inferior epigastric vessels lie between the abdominal wall muscles and the transversalis fascia.1 Because of their lateral position, they are rarely at risk during a midline approach but may be injured during a more lateral approach. Otherwise the rectus muscle can be split and the posterior sheath approached between the muscle fibers.

After the rectus muscle is swept away, the posterior rectus sheath is grasped and carefully incised to prevent cutting through the peritoneum (Figs. 27-6 and 27-7). The incision of the posterior sheath provides the entry into the retroperitoneal space. The retroperitoneal fat tissue lies between the posterior sheath and the peritoneum.

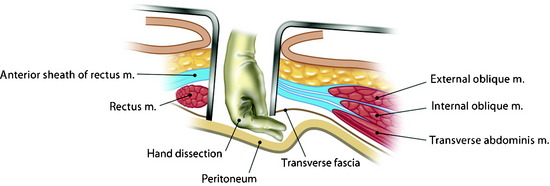
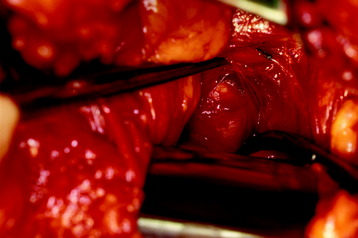
RETROPERITONEAL DISSECTION
Once the peritoneum is identified, it is swept off the abdominal wall with a blunt dissection (Figs. 27-8 and 27-9). An alternative method is to incise the fibers of the transversalis fascia below the arcuate line.2 The blunt dissection allows the surgeon to find the plane between the peritoneum and the transversalis fascia, which can be incised rostrally.
L5 BODY EXPOSURE
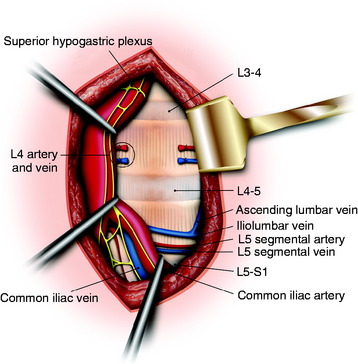
The L5 vertebral body is approached by mobilizing the great vessels at the bifurcation. Because the vascular anatomy at this level is somewhat varied, the surgeon should confirm the level of the L5–S1 disc space with an intraoperative x-ray. The bifurcation of the vena cava occurs lower than that of the aorta and is usually located above the L5–S1 disc space (Fig. 27-10).3 The aortic bifurcation usually is immediately anterior to the body of the L4 vertebrae, and the origin of the common iliac veins is observed mainly at the L5 body.
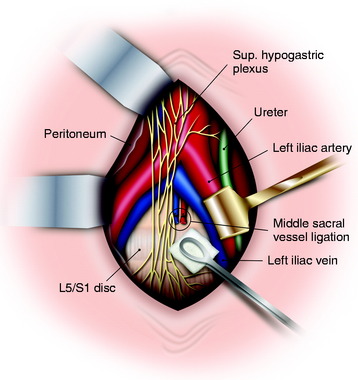
The vena cava bifurcation is to the right of the aorta, and the left common iliac vein passes through the aortic bifurcation. In the lower lumbar spine levels, care must be taken to identify all branches of the common iliac arteries and veins. The left common iliac vein, which is commonly injured, crosses at the L4–5 disc space. Ligating all branches will allow for the vessels to be mobilized to access the spine. The middle sacral artery and vein are routinely ligated during the operation to facilitate exposure. The sacral artery arises from the dorsal surface of the aorta just proximal to its bifurcation (Fig. 27-11). It is recommended that either vascular clamps or suture ligation are used to achieve this, and that the use of monopolar cautery is kept to a minimum. The use of electrocautery can cause damage to the superior hypogastric plexus, which in males can result in retrograde ejaculation.
VASCULAR MOBILIZATION
The dissection is carried anterior and medial to the left common iliac vessels. The middle sacral artery and vein may be taken with ligation. The left iliac vein needs to be widely mobilized to allow placement of the retractor against the left lateral edge of the spine.4
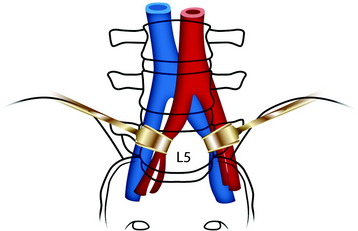
The L5 approach is easy to perform in patients with a high-lying bifurcation (Fig. 27-12). The bilateral retraction of common iliac vessels provides adequate exposure of the L5 vertebral body.
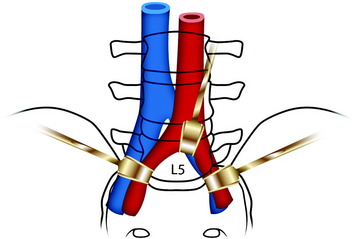
For patients with bifurcation on the L4–5 disc level, an upward retraction of the bifurcation point of great vessels is necessary (Fig. 27-13).
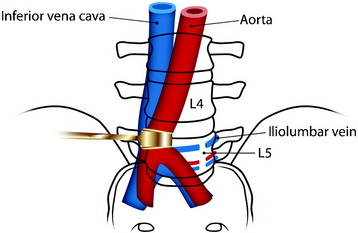
In cases of low-lying bifurcation, the retraction of the aorta and vena cava is accomplished from the left to the right side to expose the L5 vertebral body (Fig. 27-14). For the vena cava to be retracted, the iliolumbar vein and fifth lumbar vein should be searched out and ligated. The iliolumbar vein makes a tethering effect on the common iliac vein. For the L5 segmental vessels and iliolumbar vein to be found, the medial margin of the psoas muscle should be retracted to the lateral side. When the tumor infiltrates the vertebral body, the periosteum and anterior longitudinal ligament (ALL) slacken, causing adhesion between the ALL and overlying vessels. The dissection of the vessels may be difficult.
L4 BODY EXPOSURE
The great vessels and the superior hypogastric plexus are retracted in the medial direction (Figs. 27-15 to 27-17). For easy retraction of the great vessels, the L5 segmental vessels and iliolumbar vein may be ligated (see Fig. 27-15).

Before the L4 corpectomy is performed, the adjacent discs are removed. The L3–4 intervertebral disc and the L4–5 intervertebral disc are removed and the L4 vertebral body is approached. With the monopolar coagulator, the ALL is coagulated and resected (see Fig. 27-16). Vertebral body removal is performed with a punch and drill. After the posterior cortex of the vertebral body is removed, the ventral dura is seen. From the dural sac, the origin of the nerve root can be seen.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


