Chapter 22 Anterior endoscopic cervical microdecompression of disc and foramen
The standard treatment for cervical disc protrusions and foraminal stenosis ha s been anterior cervical microdecompression of the disc and foramen with or without bony fusion [1–5]. These open operations are associated with significant local morbidity [6,7], such as graft collapse, graft extrusion, hardware failure, nonfusion with resultant instability, infections, esophageal perforation with infection, and permanent pain, peripheral nerve injury, or infection at the graft donor site. Anterior cervical fusion (ACF) is associated with a 15% or greater chance of junctional disc herniation or adjacent segment disease at interspaces adjacent to fused levels [8,9].
The evolution of spinal surgery is trending toward less invasive techniques [9–16]. Advancements in microinstrumentation, fiberoptics, improved fluoroscopic imaging, and high-resolution digital video imaging endoscopy, along with the accumulation of experience in percutaneous lumbar discectomy [17–20] and spinal laser applications [20–23], have facilitated the development of anterior endoscopic cervical microdecompression (AECM) and foraminal decompression [9,14,19]. AECM, as minimally invasive surgery, does not affect the stability of adjacent vertebral segments [8–10]. Although ACF is often an unattractive treatment for patients with multiple-level disc symptoms, AECM can be safely utilized for treatment of such patients.
Treatment objectives
The primary objective of AECM is to perform decompression of the herniated cervical disc and foraminal disc. It is a minimally invasive outpatient procedure that aims to reduce tissue trauma with much less morbidity than open cervical spinal surgery [9,10,12]. There is no graft donor site to cause secondary problems, and the period of convalescence and the costs of the procedure are significantly less than those of traditional open operations.


























Instrumentation
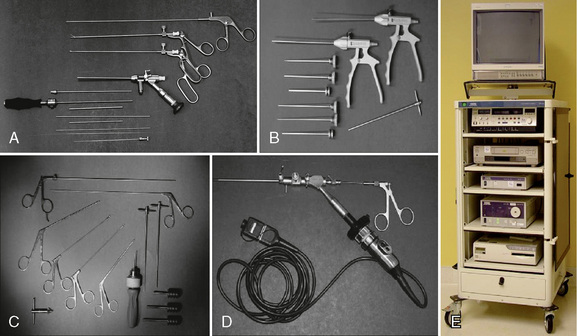
The following instruments and equipment are needed for AECM (Fig. 22-1) [9,12]:
 Endoscopic tower equipped with digital video monitor, DVT/VHS recorder, light source, photo printer, and tri-chip digital camera system.
Endoscopic tower equipped with digital video monitor, DVT/VHS recorder, light source, photo printer, and tri-chip digital camera system.





 Holmium:yttrium-aluminum-garnet (Ho:YAG) laser generator (Trimedyne, Inc., Irvine, CA) with right-angle (side-firing) probe (Fig. 22-2).
Holmium:yttrium-aluminum-garnet (Ho:YAG) laser generator (Trimedyne, Inc., Irvine, CA) with right-angle (side-firing) probe (Fig. 22-2).


Procedure





Patient Positioning
Figure 22-3 illustrates patient positioning for AECM [9,12]:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


