Chapter 37 Lateral Interbody Fusion Using the Xlif System
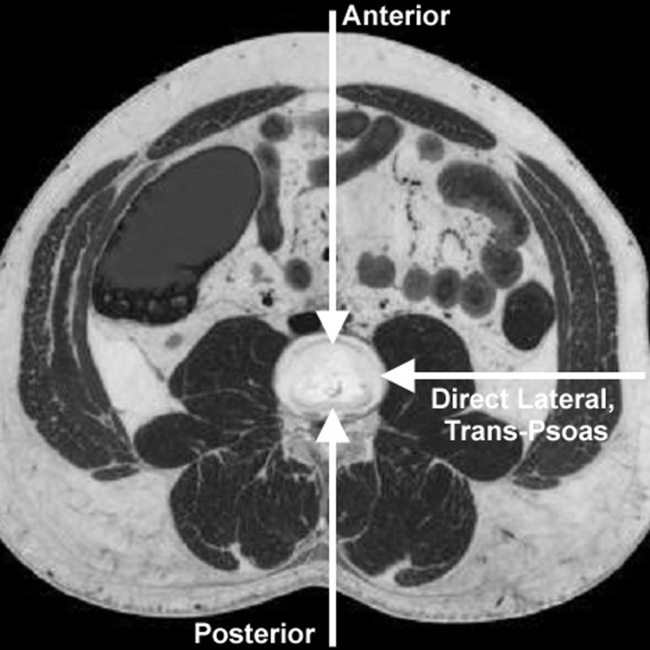
Building on the concept and technique of minimally invasive spinal approaches [1], we have developed the eXtreme Lateral Interbody Fusion (XLIF, NuVasive, Inc., San Diego, CA) approach to the lumbar spine. In contrast to the more traditional anterior lumbar interbody fusion (ALIF) method of approaching the disc anteriorly through the abdomen for implantation of cages and other devices, we have developed the XLIF technique, which accesses the disc laterally through the psoas muscle (Fig. 37-1). This approach offers adequate access to the disc space with the added benefit of reduced iatrogenic injury to abdominal vascular structures (aorta and vena cava), the sympathetic plexus (reducing incidence of retrograde ejaculation), and neural structures (namely, the spinal nerves that cross the posterior aspect of the psoas muscle). The technique employs muscle dilation through the fibers of the psoas muscle in an area approximately 3 cm in diameter.
Indications
Indications for the XLIF technique are the same as those for any interbody fusion, with the limitation of access only at disc levels above L5. Such patients typically suffer discogenic pain due to segmental instability, disc degeneration, degenerative scoliosis, and/or grade I or II spondylolisthesis [2–7]. It may also be applied to patients in whom prior decompressive surgery (i.e., discectomy and/or laminectomy) have failed and who therefore require interbody fusion, and in cases of adjacent-level disease after prior fusion surgery, because in these revision cases, scarring may limit the ability to safely perform a more traditional fusion approach. Revisions of failed interbody fusions and failed lumbar total disc replacements have also been treated with the XLIF approach for retrieval and revision.
Instrumentation
The instruments necessary for performing the XLIF procedure are as follows:
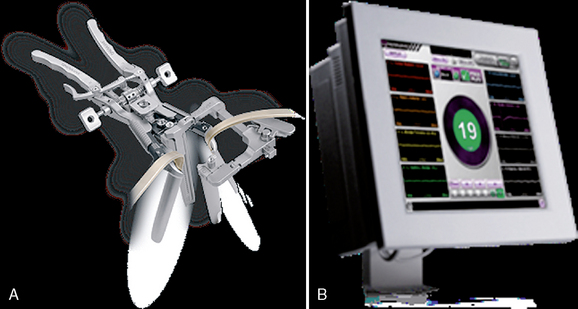
 MaXcess System of dilators and split-blade retractor (Fig. 37-2A; NuVasive, Inc.). Consists of bifurcated light cable, articulating arm, retractor system with various length blades, and blade-extension shims.
MaXcess System of dilators and split-blade retractor (Fig. 37-2A; NuVasive, Inc.). Consists of bifurcated light cable, articulating arm, retractor system with various length blades, and blade-extension shims. NeuroVision System for MaXcess-compatible stimulated and continuous electromyography (EMG) monitoring of nearby nerves (Fig. 37-2B; NuVasive, Inc.).
NeuroVision System for MaXcess-compatible stimulated and continuous electromyography (EMG) monitoring of nearby nerves (Fig. 37-2B; NuVasive, Inc.).



Surgical technique
Patient Preparation
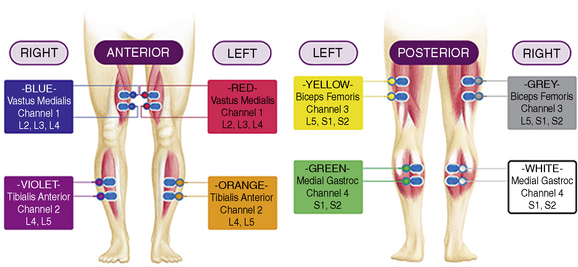
In the preoperative waiting area, the patient is prepared for NeuroVision EMG monitoring; four muscle groups per side can be monitored using the NeuroVision System. These four muscles are easily palpated and represent spinal nerve distributions from L2-S2: the vastus medialis, the anterior tibialis, the biceps femoris, and the medial gastrocnemius (Fig. 37-3). A reference electrode is also placed on the upper lateral thigh, and an anode return electrode is placed superior to the operative site, such as on the latissimus dorsi muscle.
Patient Positioning
Related posts:
 Atlantooccipital and Atlantoaxial Joint Block for Cervicogenic Headache
Posterior Lumbar Foraminal Decompression
Minimally Invasive Percutaneous Lumbar Fusion Technique
Percutaneous Endoscopic Cervical Discectomy and Stabilization
Intervertebral Discography
Transaxial Anterior Lumbar Interbody Fusion Using the AxiaLIF System
Atlantooccipital and Atlantoaxial Joint Block for Cervicogenic Headache
Posterior Lumbar Foraminal Decompression
Minimally Invasive Percutaneous Lumbar Fusion Technique
Percutaneous Endoscopic Cervical Discectomy and Stabilization
Intervertebral Discography
Transaxial Anterior Lumbar Interbody Fusion Using the AxiaLIF System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


