caution!
Although muscle disease itself leads to morbidity and even mortality, involvement of other organ systems is the usual ultimate cause of death in most patients. Consequently, when appropriate, involvement of other specialists, mostly cardiologists and pulmonologists, is critical in the care of patients with myopathies.
6. What Is the Pattern of Weakness?
Depending on the myopathy, weakness initially manifests in particular muscle groups or regions of the body including ocular, pharyngeal, facial, respiratory, axial, and proximal or distal limb muscles. Commonly, more than one of these areas is affected. By determining the pattern of muscle involvement, the differential diagnosis can be narrowed considerably.
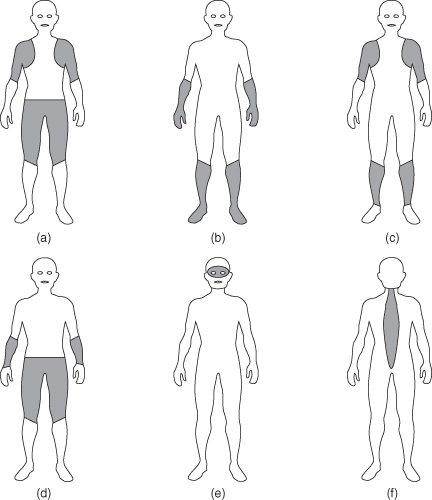
A careful examination places the patient into one of six distinctive patterns (Figure 2.1).
Figure 2.1. Patterns of muscle weakness: (a) proximal; (b) distal; (c) proximal arm with distal leg; (d) proximal leg with distal arm; (e) ptosis; and (f) axial muscles.
Proximal Arms and Legs
This “limb girdle” pattern is the one that most clinicians think of for myopathies. It is the most common and least specific pattern. Dermatomyositis, polymyositis, and most dystrophies present with this pattern, as do congenital, mitochondrial, myofibrillar, endocrine, metabolic, and toxic myopathies. However, the history should have narrowed the possibilities. Inflammatory myopathies present acutely or subacutely. Weakness from birth suggests a congenital myopathy, whereas a 6-year-old boy with a Gower sign most likely has Duchenne dystrophy. A history of recently prescribed cholesterol-lowering drugs points toward a toxic myopathy.
Distal Weakness
In these disorders, there is weakness of ankle dorsiflexion or plantar flexion, weakness of the wrists and fingers, or some combination thereof. Of the distal muscular dystrophies, Nonaka, Laing, and Miyoshi dystrophies have onset in children or young adults, whereas Markesbery–Griggs, Welander and Udd dystrophies present in middle age or older. The myofibrillar myopathies and myotonic dystrophy may also have primarily distal weakness.
Proximal Arms and Distal Legs
In this “scapuloperoneal” pattern, the periscapular muscles, along with the anterior foreleg muscles, are most affected. The scapuloperoneal, Emory–Dreifuss and facioscapulohumeral muscular dystrophies fall into this category.
Proximal Legs with Distal Arms
This is the classic pattern seen in most patients with sporadic inclusion body myositis. There is prominent weakness and wasting of the quadriceps (Figure 2.2) as well as wrist and finger flexors.
Figure 2.2. Marked atrophy of the quadriceps muscles in a patient with inclusion body myositis – note the asymmetry with greater atrophy on the left.

Ptosis and Ophthalmoparesis
Ptosis with ophthalmoplegia is characteristic of a limited number of disorders, usually oculopharyngeal muscular dystrophy or mitochondrial myopathies. Even though patients have limited extraocular movements, they rarely complain of diplopia. Ptosis without ophthalmoplegia occurs in myotonic dystrophy along with the congenital and myofibrillar myopathies.
Axial Musculature
The most prominent weakness in some patients may be of the neck (isolated neck extensor myopathy) or the paraspinous muscles (camptocormia). In isolation, these presentations may be due to muscle disease, but more often occur in disorders of the neuromuscular junction or motor neuron. Patients may also present with rigidity of the spine due not to weakness, but to contractures of the axial structures. This is commonly seen in congenital, Ullrich, and Emory–Dreifuss muscular dystrophies.
Finally, some patients remain relatively asymptomatic between attacks of weakness, stiffness, myoglobinuria, or pain, and thus do not fit into one of the above categories. Most of these patients have disorders in some way affecting components of the muscle membrane or energy pathways. Thus, the myotonias, periodic paralyses, metabolic myopathies, and drug ingestions fall into this category. However, over time, some of these may transform from episodic to progressive disorders.
Diagnostic Tests
The six questions with six patterns help narrow the diagnosis considerably and determine what diagnostic tests should follow. Creatine kinase (CK) is the most valuable laboratory test and assists in narrowing the differential diagnosis. Markedly elevated CK levels occur in dystrophies with defects in the muscle membrane such as Duchenne dystrophy, some inflammatory myopathies, hypothyroid myopathy, and rhabdomyolysis. Inversely, CK levels may be disproportionately low in very weak patients with dermatomyositis or hyperthyroidism.
 tips and tricks
tips and tricks
Resting CK levels are influenced by muscle mass, gender, and race. Although, in most labs, the upper limit of normal (ULN) ranges from 160 international units per liter (IU/L) to 240 IU/L, studies show that race and gender have to be taken into account:
| Group | Constituents | ULN (97.5%) |
| High | Black males | 520 IU/L |
| Intermediate | Nonblack males and black females | 345 IU/L |
| Low | Nonblack females | 145 IU/L |




