Approach to the Patient with Hearing Loss
Richard T. Miyamoto
Marcia J. Hay-McCutcheon
Hearing loss affects almost 17 in 1,000 children under the age of 18 and approximately 314 in 1,000 adults over the age of 65. It has been estimated that 28 million Americans have a hearing impairment. Hearing loss produces substantial communication problems and can be the presenting symptom of serious underlying medical disorders. A detailed medical and audiologic evaluation is required to establish a specific etiology and management plan.
I. ETIOLOGY
There are various and often complex causes of hearing loss. In many cases, particularly among children, the cause of the hearing loss may remain unknown or idiopathic even after an extensive medical and audiologic work-up.
A. Despite the diversity of patients and their presenting symptoms, the causes of hearing loss can be classified as hereditary or acquired. Occasionally, there is not a clear distinction between the two types. For example, there is a genetic predisposition for certain populations to be more susceptible to noise-induced hearing loss.
B. The onset of hearing loss is a useful indicator when describing the cause. Hearing loss is considered congenital when it was caused before birth, perinatal when the hearing loss occurs during birth or shortly thereafter, and postnatal when the onset of the hearing loss occurs more than a month after birth.
C. Nonorganic hearing loss may occur in children and adults and its prevalence varies depending on the clinical situation.
II. ANATOMY AND PHYSIOLOGY OF THE AUDITORY SYSTEM
The auditory system is divided into four anatomical regions: (1) the external ear, (2) the middle ear, (3) the inner ear, and (4) the central auditory pathway.
A. The external ear consists of the pinna and the external auditory canal. It collects and directs sound to the tympanic membrane. Because of its physical dimensions, the external ear provides an important resonance boost between 2,000 and 5,000 Hz, a frequency range that contributes to the perception of speech.
B. The middle ear consists of the tympanic membrane, three ossicles (malleus, incus, and stapes), two middle ear muscles (tensor tympani and stapedius), and the ligaments that suspend the ossicles in the middle ear cavity. The middle ear structures transmit acoustic energy from the external environment to the inner ear and serve as a mechanical transformer recovering energy that would otherwise be lost as sound is transmitted from a gaseous medium (air) to a liquid medium (endolymph). The middle ear structures compensate for this impedance mismatch between the air and liquid mediums. Specifically, the difference in the areal ratio between the relatively large tympanic membrane and the small oval window recovers a substantial portion of the energy lost. Additionally, energy is recovered through the lever action of the handle of the malleus; that is, the handle is slightly longer than the long process of the incus.
C. The inner ear is divided into the vestibular portion consisting of three semicircular canals as well as the utricle and saccule, and the auditory portion consisting of the cochlea. The semicircular canals provide information regarding angular acceleration, and
the utricle and saccule provide information regarding gravitational or linear acceleration. The vestibular system, coupled with the visual and proprioceptive systems, functions as the body’s balance mechanism. The cochlea is the end organ of hearing and is a shellshaped cavity placed within the bony labyrinth. This fluid-filled structure is divided into three sections via the basilar membrane and Riessner’s membrane. These sections are the scala vestibuli, the scala media (housing the hair cells), and the scale tympani. With the displacement of the stapes, a wave of motion (i.e., traveling wave) moves up the basilar membrane resulting in displacement of the one row of inner hair cells and three rows of outer hair cells. Sitting on the top of the hair cells are tiny cells referred to as stereocilia, which make direct contact with the tectorial membrane, a structure directly above the hair cells. The shearing action of the stereocilia on the tectorial membrane results in the stimulation of the hair cells. This motion causes the opening and closing of channels, which allows ions to flow into and out of the hair cells, thereby beginning the neural transduction process. The stiffness and mass characteristics of the basilar membrane vary along its length, and therefore, the traveling wave envelope will reach a peak at different locations. This location corresponds to a specific frequency region equivalent to the frequency of the auditory stimulus. Thus the inner ear acts as a low-pass filter with high-frequency sounds encoded at the basal region of the cochlea and low-frequency sounds encoded at the apical region of the cochlea. This tonotopic arrangement is maintained throughout the central auditory system.
the utricle and saccule provide information regarding gravitational or linear acceleration. The vestibular system, coupled with the visual and proprioceptive systems, functions as the body’s balance mechanism. The cochlea is the end organ of hearing and is a shellshaped cavity placed within the bony labyrinth. This fluid-filled structure is divided into three sections via the basilar membrane and Riessner’s membrane. These sections are the scala vestibuli, the scala media (housing the hair cells), and the scale tympani. With the displacement of the stapes, a wave of motion (i.e., traveling wave) moves up the basilar membrane resulting in displacement of the one row of inner hair cells and three rows of outer hair cells. Sitting on the top of the hair cells are tiny cells referred to as stereocilia, which make direct contact with the tectorial membrane, a structure directly above the hair cells. The shearing action of the stereocilia on the tectorial membrane results in the stimulation of the hair cells. This motion causes the opening and closing of channels, which allows ions to flow into and out of the hair cells, thereby beginning the neural transduction process. The stiffness and mass characteristics of the basilar membrane vary along its length, and therefore, the traveling wave envelope will reach a peak at different locations. This location corresponds to a specific frequency region equivalent to the frequency of the auditory stimulus. Thus the inner ear acts as a low-pass filter with high-frequency sounds encoded at the basal region of the cochlea and low-frequency sounds encoded at the apical region of the cochlea. This tonotopic arrangement is maintained throughout the central auditory system.
D. Central auditory system. The central auditory system consists of the auditory portion of the eighth cranial nerve, the cochlear nucleus, the trapezoid body, the superior olivary complex, the lateral lemniscus, the inferior colliculus, the medial geniculate body of the thalamus, and finally the auditory cortex. The level of neural complexity increases exponentially with each higher order neuron or central auditory nucleus.
III. MEDICAL EVALUATION
Evaluation of the auditory system is accomplished by obtaining a detailed history, performing a physical examination, and conducting audiologic tests. In selected cases, radiologic imaging may be indicated.
A. History.
The otologic history includes inquiry into symptoms of ear disease, including hearing loss, ear pain (otalgia), discharge from the ear (otorrhea), tinnitus or other head noises, and vertigo or dizziness. If any of these symptoms are present, a detailed characterization is performed. The clinical significance of hearing loss is related to the time and acuity of onset, severity, and the tendency to fluctuate or progress. The deleterious effects of hearing loss are particularly great when the onset occurs before the development of spoken language (i.e., prelingual hearing loss).
B. Physical examination.
1. The otologic examination begins with inspection of the pinna and palpation of periauricular structures, including the periauricular and parotid lymph nodes.
2. Otoscopic examination of the external ear canal and tympanic membranes is performed to identify abnormalities of these structures. Pneumatic otoscopy is helpful in assessing the mobility of the tympanic membrane and is particularly useful in identifying a subtle middle ear effusion.
3. A complete head and neck examination is performed, including a cranial nerve and cerebellar testing.
4. Tuning fork tests are an important part of the otologic functional examination for hearing acuity. They are particularly useful in differentiation between conductive and sensorineural hearing loss. The most useful tuning forks are those with vibrating frequencies of 512 and 1,024 cycles per second. The 2 most commonly used tuning fork tests are Weber’s test and Rinne’s test.
Weber’s test is performed by placing the stem of the tuning fork on the midline plane of the skull. The patient is asked to identify the location of the auditory percept within the head. The signal lateralizes to the ear with conductive hearing loss provided normal hearing is present in the opposite ear. This occurs because the ambient
room noise present in the usual testing situation tends to mask the normal ear, but the poorer ear with a conductive loss does not hear such noise and better hears boneconducted sound. If a sensorineural loss is present in one ear and the opposite ear is normal, the fork is heard louder in the better ear.
Rinne’s test is performed by alternately placing a ringing tuning fork opposite one external auditory meatus and firmly on the adjacent mastoid bone. The loudness of the tuning fork in these two locations is compared. The normal ear hears a tuning fork about twice as long with air conduction as with bone conduction. Conductive hearing loss reverses this ratio, and sound is heard longer with bone conduction than with air conduction. Patients with sensorineural hearing loss hear better by means of air conduction than by means of bone conduction, although hearing is reduced with both air and bone conduction.
IV. AUDIOLOGIC EVALUATION
The audiologic evaluation characterizes the type, severity, and configuration of a hearing loss. Loss of hearing can be either partial or total. It can affect the low, middle, or high frequencies in any combination.
A. Range of hearing.
Although the human ear is sensitive to frequencies between 20 and 20,000 Hz, the frequency range from 300 to 3,000 Hz is most important for understanding speech.
1. During an audiologic evaluation, pure-tone thresholds are routinely obtained for frequencies at octave intervals between 250 and 8,000 Hz.
2. The range of sound pressure to which the human ear responds is immense. Infinitesimal movement of the hair cells produces a just audible sound, yet a million-fold increase is still tolerable.
3. The large range of numbers needed to describe audible sound pressure is best represented by a logarithmic ratio comparing a sound to a standard reference sound. This is called the decibel. The decibel is defined in relation to the physical reference of sound, or sound pressure level, to the average threshold of normal hearing for young adults, or hearing level (HL), or to a patient’s own threshold for the sound stimulus, or sensation level.
4. Speech sounds vary in their acoustic characteristics. Vowels tend to have most of their energy in the low to middle frequencies and are produced at relatively higher intensities than consonants. Thus vowels carry the power of speech. Consonants tend to contain higher frequency information and have low power. Much of the actual understanding of speech depends on the correct perception of consonants. Consequently, speech may not be audible for patients with hearing loss across the entire frequency range. Patients with hearing loss in the higher frequencies may hear speech but not understand it.
B. Audiogram.
To graphically represent the degree of hearing, pure-tone thresholds are displayed on an audiogram (Fig. 17.1). On this graph, frequency (pitch) is represented on the horizontal axis and intensity (loudness) is presented on the vertical axis. The 0 dB HL line represents the average threshold level for a group of normal-hearing young adults with no history of otologic disease or noise exposure. Conversational speech at a distance of 1 m has an intensity level of approximately 50 to 60 dB HL. Speech becomes uncomfortable to listen to at approximately 80 to 90 dB HL.
C. Pure-tone threshold audiometry.
The audiometric threshold is defined as the softest intensity level of a pure-tone signal that can be detected by the patient 50% of the time. Thresholds are generally obtained for air-conduction stimuli presented through earphones or in a sound field, and for bone-conduction stimuli presented with a vibrator placed on the mastoid or forehead.
For adults and older children, pure-tone testing simply requires a behavioral response to pure-tone stimulation. For infants older than 5 months, visual reinforcement audiometry can be used to obtain thresholds. In this operant discrimination task (i.e., yes-no paradigm), infants are trained to turn to their right or left when they hear a signal, where they see an illuminated animated toy. Alternatively, play audiometry is used to assess the hearing of preschool children. In this technique, play activities are used as operant reinforcers for a child’s response to auditory signals.
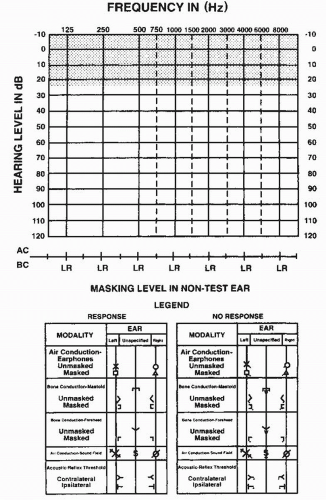 FIGURE 17.1 A sample audiogram. The y–axis represents the intensity level in dB HL and the x–axis represents the pure-tone frequency of the stimulus. The threshold is the softest level that the patient hears the pure-tone signal 50% of the time. |
Related posts:
 Approach to the Patient with Gait Disturbances and Recurrent Falls
Approach to the Patient with Gait Disturbances and Recurrent Falls
 Approach to the Hyperkinetic Patient
Approach to the Hyperkinetic Patient
 Approach to the Patient with Lower Extremity Pain, Paresthesias, and Entrapment Neuropathies
Approach to the Patient with Lower Extremity Pain, Paresthesias, and Entrapment Neuropathies
 Approach to the Patient with Chronic and Recurrent Headache
Approach to the Patient with Chronic and Recurrent Headache
 Epilepsies in Children
Epilepsies in Children
 Neuroimaging of Common Neurologic Conditions
Neuroimaging of Common Neurologic Conditions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


