Chapter 133 Arachnoiditis and Syringomyelia
Syringomyelia can develop secondary to many pathologic processes such as Chiari malformations, spine tumors, cysts, traumatic events, spinal deformities, and arachnoiditis. All these conditions likely share a common pathophysiologic disruption of cerebrospinal fluid (CSF) flow regulation.1,2 This chapter focuses solely on syringomyelia derived from spinal arachnoiditis, excluding traumatic etiologies. Spinal adhesive arachnoiditis has been associated most commonly with postsurgical inflammation, myelography, and infection. However, rare cases of idiopathic arachnoiditis, arachnoiditis after spinal subarachnoid hemorrhage, and familial arachnoiditis have also been reported.3–5
The first clinical presentation of syringomyelia was described by Portal in 1804.6 However, the first case of cervical spinal cord cavitation secondary to arachnoiditis was probably described in 1861 by Vulpian from a necropsy.7 The first treatment was performed by Abbe and Coley in 1892 as drainage of a postmeningitic syrinx.8 Subsequently, more clinical cases attributed to postsyphilitic inflammation were published.9 The first association between degenerative disc disease and arachnoiditis was largely attributed to French in 1946.10 Although theories about the pathologic process and causative agents have evolved, treatment of arachnoiditis has improved little over the years.
Epidemiology and Definition
Spinal adhesive arachnoiditis (SAA) describes the scarring of pia and arachnoid membranes within the thecal sac. Although the pathophysiology remains elusive, thickening and adhesion of pia and arachnoid membranes are thought to arise secondarily from chronic inflammation. SAA can range from mild focal adhesions to severe scarring as is seen with arachnoid ossificans. SAA seems to have a predilection for the lumbar spine (up to 86% in some series), although this may simply reflect a predominance of postmyelographic arachnoiditis in the literature.11 The diagnosis of arachnoiditis is confirmed radiographically by using MRI or myelography. The disease spectrum varies considerably from focal scarring or slight nerve root sheath changes to dense scarring throughout the spinal axis. Variations in defining the severity of arachnoiditis likely influence the reported incidence.
Risk factors are largely inherent in the varying underlying pathologic processes that cause inflammation (Box 133-1). Infection, subarachnoid hemorrhage, degenerative lumbar disease, history of myelography, prior lumbar anesthesia, prior spine surgery, transverse myelitis, prior baclofen pump insertion, and even intrathecal steroid injection have all been postulated as causative triggers leading to the development of spinal adhesive arachnoiditis.12–18 Infectious etiologies include tuberculous meningitis, pyogenic infections, cysticercosis, candida tropicalis, chromoblastomycosis, cryptococcosis, listeriosis, and syphilis.9,19–23 Some studies have suggested that the addition of blood products to contrast agents in myelography contributed to the increased risk of arachnoiditis. No study has evaluated whether durotomies or synthetic sealants used to reinforce durotomy closures influence the risk of developing arachnoiditis.
Box 133-1 Etiologies of Arachnoiditis
Several series have estimated the incidence of lumbar postmyelography arachnoiditis and symptomatic fibrosis to be near 1%.24 However, published data on postmyelography arachnoiditis are limited by the use of varying contrast agents and a variable time to presentation. For example, one study reported the development of syringomyelia 44 years after myelography.25 Some series have found asymptomatic but radiographic signs of arachnoiditis in 16.5% to 35% of patients after myelography.26 However, other studies suggest a lower incidence in the absence of surgical intervention with myelography alone. Laitt et al. reported that 62.4% (68 of 109) of their patients had some degree of arachnoiditis after Myodil myelography, but 50 of their patients had prior lumbar surgery.27 The incidence was only 3% in patients with myelography alone, whereas arachnoiditis was present in 88% of people who had prior lumbar surgery and myelography.
Failed back syndrome is an entity that is familiar to most surgeons. Some series have estimated that 6% to 16% of patients who have had prior spine surgery develop some degree of arachnoiditis contributing to persistent pain. Fitt and Stevens found 20% (26 of 129) of patients with a history of lumbar surgery to have some degree of arachnoiditis.28 Many studies have grouped epidural scarring and intradural pathology such as arachnoiditis together in their evaluations; therefore, the incidence of arachnoiditis alone is likely overreported in the literature.29 Burton reported that 11% of their failed back surgeries were due to arachnoiditis. Several studies have clearly associated an increased risk of arachnoiditis developing in patients who have undergone prior spine surgeries.27,30 Certainly, arachnoiditis should be considered in managing postoperative patients with persistent or recurrent symptoms.
Pathophysiology of Arachnoiditis-Associated Syringomyelia
Although no definitive pathologic mechanism of arachnoiditis-associated syringomyelia has been elucidated thus far, several different theories have been postulated. One of these theories speculates that the blood products from myelography act as a catalyst coating oil drops in fibrin, thus emulsifying them and contributing to the development of severe arachnoiditis.31 Several other authors propose that an initial minor trauma or local irritants such as contrast-myelography could serve as causative agents that trigger an inflammatory response.17,25 McLean et al. hypothesize that tethering of the spinal cord from arachnoiditis causes repeated compression along the spinal cord with normal physiologic movements leading to pathologic injury.32,33
Another theory postulates that syringomyelia associated with arachnoiditis is secondary to formation of microcysts that develop within the spinal cord from ischemic injury. The impaired CSF flow from the arachnoiditis contributes to intramedullary cystic degeneration from ischemia due to circulatory disturbance in the pia-arachnoid, which would coalesce into a syrinx.34,35
Williams and Bentley created a syringomyelia model in dogs by injecting kaolin in the cisterna magna and causing significant arachnoiditis.36 They noted that typical findings associated with ischemia were absent in their pathologic specimens. However, whether their model truly mimics the pathology that is seen in human arachnoiditis remains unclear, as all their specimens had a patent fourth ventricular communication with the syrinx.
Alternatively, other researchers argue that the increased CSF pressure differential from an obstruction leads to direct communication of CSF via Virchow-Robin spaces into the spinal cord that forms a syrinx.37,38 Alternative drainage pathways that have been hypothesized include the dorsal root entry zone and perivascular channels.39,40
A more recent hypothesis that has growing support from various studies is that extracellular fluid from interstitial edema contributes to the formation of a syrinx secondary to the scarring of the pia-arachnoid. The scarring of the pia-arachnoid is thought to impair some degree of CSF absorption while increasing venous stasis, thus increasing the amount of interstitial fluid.41 This theory has been supported by animal and mathematical models that obstruct the CSF space, leading to development of edema and possibly a “pre-syrinx” state.42,43 Yet another hypothesis incorporates pressure dissociation above and below the obstruction with disruption along the blood–spinal cord barrier leading to ultrafiltration of protein-poor fluid into a syrinx.44
Hypotheses explaining the development of syringomyelia have ranged from hydrodynamic theories to pressure dissociation theories involving accumulation of extracellular fluid.35,44,45 However, we still have an incomplete understanding of the pathophysiologic process that leads to syringomyelia formation.
Radiographic Findings of Arachnoiditis
With the advent of myelography, lumbar arachnoiditis has been described as nerve root clumping, contraction of the thecal sac, an appearance of an empty or thickened thecal sac, short/blunted perineural sheathes, or obliteration of nerve root sheathes.46 Wilkinson further classified these findings into grades of severity47:
1. Unilateral defect on the nerve root exit pouch adjacent to the disc
2. Circumferential or anular defect with bilateral notch and filiform passage of contrast medium
3. Complete transverse obstruction with “stalagmites,” candle-guttering, or paintbrush defects
4. Infundibulum cul-de-sac, loss of radicular striation, cutting off of root sleeves
However, with the advent of MRI, less invasive imaging studies were available. Ross and Delamarter summarized their MRI findings into a classification with 92% sensitivity, 100% specificity, and 99% accuracy (Table 133-1). Classification of MRI findings associated with lumbar arachnoiditis48,49:
1. Conglomeration of nerve roots centrally located, no enhancement
2. Nerve roots attached laterally/clumped with meningeal thickening
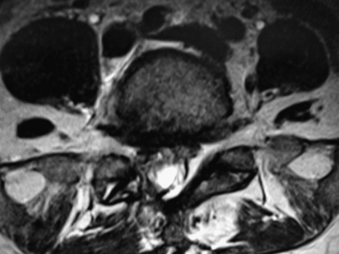
3. “Empty thecal sac” appearance (Fig. 133-1)
4. Soft tissue mass within the canal obliterating subarachnoid space
Table 133-1 MRI Findings Associated with Lumbar Arachnoiditis
| Grade | MRI Findings |
|---|---|
| 1 | Conglomeration of nerve roots centrally located, no enhancement |
| 2 | Nerve roots attached laterally, clumped with meningeal thickening, “empty thecal sac” appearance |
| 3 | Soft tissue mass within canal obliteration of subarachnoid space |
Ross and Delamarter’s definitions are commonly used, although other authors have further simplified their findings into even fewer categories. Jorgensen et al. divided MRI findings into two categories50:
1. Adhesion of roots inside meninges, “sleeveless” appearance (Ross and Delamarter types 1 and 2)
2. Thecal sac changes, filling defects/narrowing/shortened/occlusion (Ross and Delamarter type 3)
Usually, MRI is adequate to confirm the diagnosis of arachnoiditis,28,51 but some cases are quite subtle and might not be as evident on MRI. Brodbelt and Stoodley described three cases in which a mild, single arachnoid web was sufficient to cause CSF flow impairment.14 Some authors have advocated that constructive interface steady state images are better suited to visualize dural thickening, syringomyelia, microcystic lesions, and deformity of the cord, but less adequate to identify “pre-syrinx” findings.52 Myelography can be invaluable to identify small areas of CSF flow obstruction that are responsible for symptoms.
It is important to note that lumbar spinal stenosis in itself is often associated with radiographic findings that resemble Delamarter type 1 clumping of nerve roots and should be distinguished from arachnoiditis based on the clinical history.53 These findings are likely due to mechanical pressures from the stenosis as opposed to arachnoid/pial fibrosis as seen in arachnoiditis.
Clinical Presentation and Clinical Course
Patients typically present with slowly progressive, chronic symptoms. The symptomatology is largely defined by the anatomic location of the pathology. Given that lumbar arachnoiditis is more prevalent, a greater percentage of patients initially present with lumbar radiculopathy, sensory deficits, and back pain.54,55 Eventually, patients develop more objective findings of decreased reflexes and motor deficits progressing to bowel and bladder dysfunction, essentially a cauda equina syndrome.55 These patients often have a history of an invasive lumbar procedure, either myelography, surgery, or even a percutaneous injection for pain control. Alternatively, patients who develop cervicothoracic arachnoiditis present with myelopathy secondary to spinal cord compression (Figs. 133-2 to 133-5). Thoracic myelopathy is more commonly encountered, but cervical cases have been described.

Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


