Fig. 1
Upper left: Surgical approaches according to height of bifurcation or neck of basilar distal aneurysm relative to posterior clinoid. Upper right: Surgical routes for the distal basilar aneurysms when pterional craniotomy is selected. Lower left: Intra-operative photographs of Case 1. Lower right: Intra-operative photographs of Case 2
BA-bif and BA-SCA aneurysms can be approached using pterional craniotomy. A basilar top complex that looks like a dragonfly appears when Liliequist’s membrane is opened, and the optimal route to the aneurysm’s neck, lateral to internal carotid artery (ICA), medial to ICA, or posterior to ICA, is selected (Fig. 1, upper right).
There are several tips for clipping distal BA aneurysms [1]. Superficial Sylvian and frontobasal veins must be preserved. Proximal control at the proximal BA should be prepared, in particular, when the height of the neck is low or the size of the aneurysm is large. It is very useful to soften the dome during neck dissection and clip placement. For emergent control for intra-operative rupture, proximal control of BA is absolutely necessary. For this purpose, posterior clinoidectomy is sometimes carried out. The drilling during the posterior clinoid process must be done meticulously. Retraction or division of the anterior tentorium is sometimes effective for proximal control of BA. Perfect clipping must be carried out after the BA-complex is confirmed. After surgical clipping, it is important to verify that the aneurysm is excluded, perforators are patent, and P1 and SCA are patent.
Several representative cases are shown here.
Case 1 is a 60-year-old female who suffered from a subarachnoid hemorrhage (SAH). Her clinical grade was IV according to WFNS grading. Surgical clipping for BA-bif An was carried out 10 days after the onset of SAH (Fig. 1, lower left).
Case 2 is a 65-year-old female who suffered from SAH. First, endovasucular coiling was carried out. Follow-up angiograms revealed a neck remnant, so clipping for BA-bif aneurysm was performed (Fig. 1, lower right).
Case 3 is a 65-year-old female who suffered from SAH; a ruptured distal anterior cerebral artery aneurysm was successfully clipped. Surgical clipping for an unruptured BA-bif aneurysm was carried out (Fig. 2, upper left).
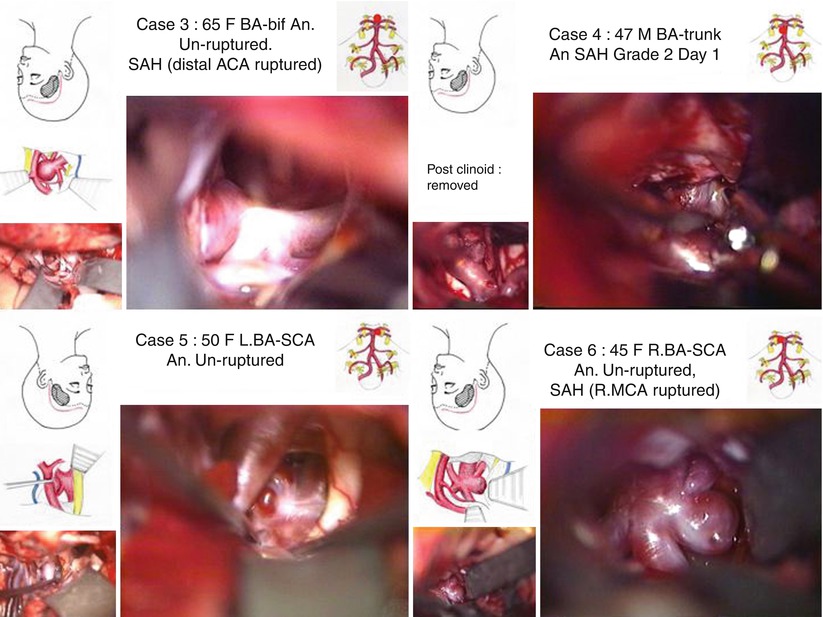
Fig. 2
Upper left: Intra-operative photographs of Case 3. Upper right: Intra-operative photographs of Case 4. Lower left: Intra-operative photographs of Case 5. Lower right: Intra-operative photographs of Case 6
Case 4 is a 47-year-old male who suffered from SAH. His clinical grade was II according to WFNS grading. Surgical clipping for a BA-trunk aneurysm was carried out 1 day after the onset of SAH (Fig.2, upper right). In this case, posterior clinoidectomy was carried out.
Case 5 is a 50-year-old female. Surgical clipping was done for her unruptured L.BA-SCA aneurysm (Fig. 2, lower left)Related posts:
 of Combined Coiling and Neuroendoscopy in the Treatment of Intraventricular Hemorrhage Due to Ruptured Aneurysm
of Combined Coiling and Neuroendoscopy in the Treatment of Intraventricular Hemorrhage Due to Ruptured Aneurysm
 Endarterectomy for Pseudo-occlusion of the Cervical Internal Carotid Artery
Endarterectomy for Pseudo-occlusion of the Cervical Internal Carotid Artery
 Mini Supra-orbital Approach for Cerebral Aneurysm of the Anterior Portion of the Circle of Willis
Mini Supra-orbital Approach for Cerebral Aneurysm of the Anterior Portion of the Circle of Willis
 Bypass Technique for Contemporary Revascularization of Unilateral MCA and Bilateral Frontal Territories in Moyamoya Vasculopathy
Bypass Technique for Contemporary Revascularization of Unilateral MCA and Bilateral Frontal Territories in Moyamoya Vasculopathy
 Bypass Using Short Interposition Vein Graft
Bypass Using Short Interposition Vein Graft
 of Plaque Location Using Indocyanine Green Videoangiography During Carotid Endarterectomy
of Plaque Location Using Indocyanine Green Videoangiography During Carotid Endarterectomy

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


