♦ Preoperative
Evaluation and Planning
- Consider a duplex ultrasound of the neck
- Magnetic resonance angiogram/computed tomographic angiogram of the neck
- Strongly recommend arteriography; according to NASCET methodology, percent stenosis is measured by percent stenosis = 1 – N/D × 100 (where N is the linear diameter at the region of greatest narrowing and D is the greatest diameter of the normal arteries distal to the carotid bulb)
- Also consider medical work-up for risk stratification and concurrent medical comorbidities
Special Operative Equipment
- Carotid endarterectomy instruments
- Well balanced vascular pick-ups
- Dissecting scissors
- Micro ring tip forceps
- Cross clamps
- Shunt clamps
- Potts scissors
- Micro-type needle drivers
- Indwelling shunt
Operating Room Set-up
- 3.5 × loupes
- Monopolar cautery
- Bipolar cautery
- Headlamp
- The patient is placed in the supine position with the head extended and turned slightly away from the site of the operation.
- Folded sheets or pillow cases should be placed beneath the shoulder blades to aid in extension of the neck as needed.
- Leads should be placed on the head by the electroencephalogram (EEG) technologist. Additionally, monitoring with somatosensory evoked potential may be considered.
♦ Intraoperative
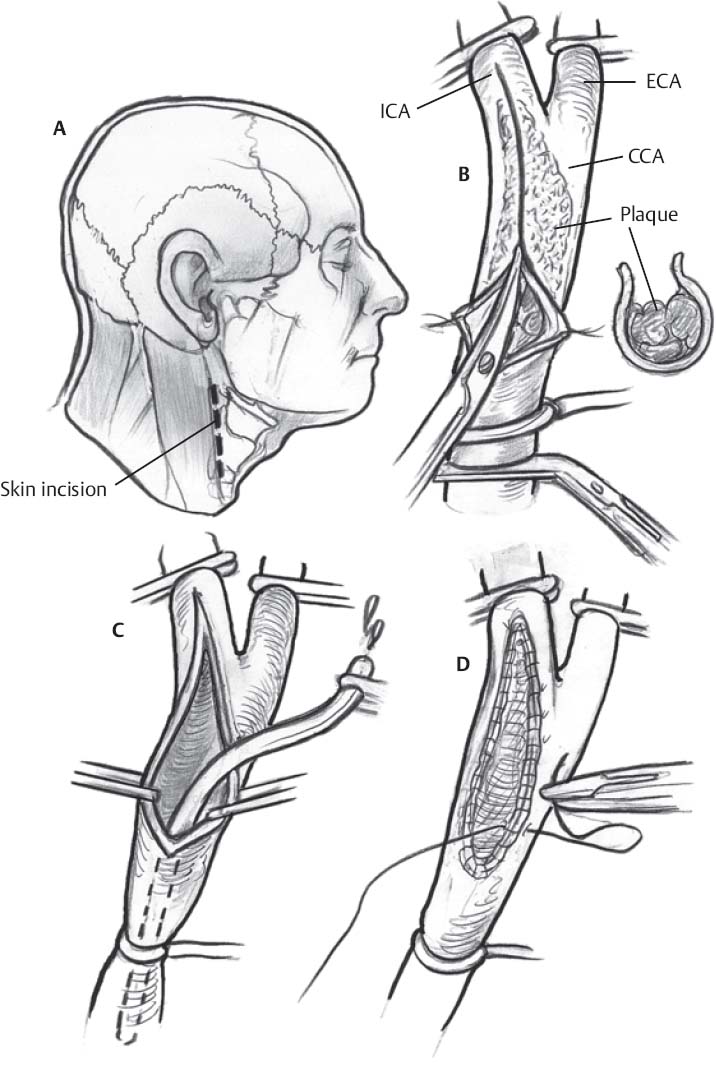
- After the patient is positioned, a linear incision is made along the anterior border of the sternocleidomastoid muscle, which may extend as high as the retroauricular region and as low as the suprasternal notch (Fig. 33.1A).
- The skin and subcutaneous tissues are then dissected sharply down through the platysma, inevitably transecting the transverse cervical nerve. Meticulous hemostasis is obtained.
- The anterior edge of the sternocleidomastoid muscle is located and retractors are placed.
- Attention is directed to the middle of the incision where dissection proceeds down the sternocleidomastoid muscle and internal jugular vein is reached and identified. Caution should be taken to avoid injuring the spinal accessory nerve. The jugular vein typically lies lateral, parallel, and slightly anterior to the internal carotid artery (ICA) and common carotid artery (CCA). The medial jugular vein is fully exposed and the jugular is retracted using a blunt blade.
- The facial vein and several smaller veins are usually doubly ligated and divided. The common facial vein is an important landmark as it crosses the field in the region of the carotid bulb.
- Afterward, 5000 units of intravenous heparin is given.
- Individual vessels are dissected out and circled with silk ties or vessel loops. If significant vital sign changes occur, 1% lidocaine may be given via a 25-gauge needle to the carotid sinus.
- The CCA and external carotid artery (ECA) are dissected circumferentially where 0 silk ties are placed around them. They are not, however, dissected free of tissue along their back walls to minimize kinking of the vessels. The ICA is freed posteriorly.
- A Rummel tourniquet is used with a 0 silk tie that passes around the CCA. Mosquito clamps are used to secure the ECA and ICA ties, which are placed with a baby right angle clamp.
- Superior thyroid artery is dissected out of the surrounding connective tissue and a double loop 00 silk ligature is placed around the vessel. Mosquitos are placed around each of the ties to keep them taught. Care must be taken to keep the field uncluttered.
Cross-clamping of the Carotid
- Cross-clamping should only occur after the ICA is dissected beyond the distal border of the plaque. Additionally, the hypoglossal nerve should be recognized high in the carotid sheath, swinging medially. This should be mobilized and gently retracted from the field using a vessel loop.
- A small ECA branch to the sternocleidomastoid muscle may require ligation to facilitate mobilization of the hypoglossal nerve.
Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


