21 Carpal Tunnel syndrome A 51-year-old, left-handed homemaker presented with a 2- to 3-year history of progressively worsening paresthesias, numbness, and tingling in the lateral three digits and radial palm of both hands, with the left hand more severely affected. She described complete left-hand numbness after peeling potatoes, and shaking the hand relieved it to some extent. She also described nocturnal numbness and burning, particularly when sleeping with her left hand flexed under her cheek, that often awakened her from sleep. These nocturnal symptoms improved slightly after she began to use wrist splints. She had recently noted difficulty in opening jars with her left hand. She denied any neck pain or radicular symptoms in the arms. Her past medical history was significant only for hypothyroidism, and her only current medication was levothyroxine. Physical examination showed a slight decrease in muscle power in the left abductor pollicis brevis. Reflexes were normal and symmetric. Sensory examination revealed decreased sensation to light touch and pinprick in the lateral three digits of both hands. Tinel sign was positive at both wrists, and a positive Phalen sign was present on the left. The remainder of the neurological examination was normal. Bilateral median nerve conduction studies revealed prolonged distal sensory and motor latencies, compatible with severe left-sided and moderate right-sided carpal tunnel syndrome (CTS). Because the patient’s paresthesias and pain failed to resolve with conservative therapy consisting of splinting and oral nonsteroidal anti-infl ammatory drugs (NSAIDs), she decided to undergo carpal tunnel release. A left carpal tunnel release was performed under local anesthesia. Operative findings included a thickened transverse carpal ligament and a swollen, indurated, and erythematous median nerve at the point of compression under the ligament. Five weeks postoperatively, the incision was well healed, and the patient described a decrease in pain, numbness, and paresthesias in her left hand. Neurological examination was normal. She continued to experience numbness and burning pain in the right hand, which did not respond to local corticosteroid injection. She agreed to consider a right carpal tunnel release in the near future. Carpal tunnel syndrome The median nerve originates from the medial and lateral cords of the brachial plexus. Coupled with the brachial artery, it runs along the medial intermuscular septum to enter the antecubital fossa medial to the biceps tendon. It enters the forearm between the two heads of the pronator teres muscle and courses along the inferior flexor digitorum sublimis (FDS) muscle belly, giving branches to the pronator teres, flexor carpi radialis, flexor digitorum superficialis, and palmaris longus. At the level of the elbow, the anterior interosseous nerve forms to innervate the flexor digitorum profundus of digits two and three, the flexor pollicis longus, and the pronator quadratus. In the distal forearm, the median nerve travels under the tendon of the palmaris longus and under the transverse carpal ligament (TCL) to enter the wrist. The TCL, an annular pulley of the flexor mechanism, is a thick fibrous band arching over the carpal bones, attaching radially to the trapezium and scaphoid tuberosity and ulnarly to the pisiform and hook of the hamate. The floor of the tunnel is composed of the volar radiocarpal ligament, as well as the bridging ligaments between the carpal bones. In addition to the median nerve, the carpal tunnel contains nine long flexor tendons, the synovium beneath the TCL, and a median nerve vascular bundle. The nerve emerges at the distal border of the TCL, where the recurrent motor branch arises to innervate the thenar muscles. To protect this structure during exposure and division of the TCL, the surgeon must be aware of the anatomical variations of the motor branch. Lanz has provided a classification of the branching variants as extraligamentous and recurrent (50%), subligamentous (30%), and transligamentous (20%). Multiple accessory motor branches may also occur as a separate variant. Sensory branches of the median nerve innervate the lateral three digits and the radial half of the fourth digit, the dorsal aspect of these digits beyond the distal interphalangeal (DIP) joint, and the radial palm. The surgeon must also aim to preserve the palmar cutaneous branch, which supplies sensation to the base of the thenar eminence. This sensory branch arises in the distal third of the forearm and does not usually enter the carpal tunnel. Instead, it courses superficial to the TCL to innervate the palmar skin. Thus, if numbness in the distribution of the palmar cutaneous branch occurs, the neuropathy is almost always above the level of the TCL, and CTS can be excluded. Only in rare branching variations will the palmar cutaneous branch pass through its own short tunnel in the TCL. The classically described presentation of CTS consists of tingling, aching, burning, or numbness of the radial half of the hand and the lateral three digits, although often the entire hand is involved. Nocturnal hypesthesias are common, often awakening the patient from sleep, when the numb hand must be shaken for the patient to obtain relief. Clumsiness or weakness of the involved hand can occur, and along with the sensory disturbances, is usually aggravated by activity or use of the hand. The onset of symptoms is usually slow and insidious, although it may be acute following a traumatic injury. Patients may occasionally present with shoulder or upper arm pain, or radiation of dysesthesias from the wrist to the proximal forearm. Most authors describe a female preponderance for CTS, with a female to male ratio of more than 2:1. Palmer has estimated an incidence of 1% in the general population, and a greater than 5% incidence among workers in industries that require repetitive use of the hands or wrists. Repetitive strain injuries represented 48% of all reported workplace illnesses in 1990, compared with 18% in 1980, with CTS ranked as the most prevalent of these disorders. More than 50% of all cases occur between the ages of 40 and 60. Early signs of the syndrome include those described by Phalen and Tinel, in which lancinating paresthesias in the median nerve distribution are reproduced by forced wrist flexion, or percussion over the median nerve at the wrist, respectively. Caveats with these supposedly pathognomonic signs include a high false-positive rate of Tinel sign and the absence of Phalen sign in patients with profound sensory loss. As the entrapment neuropathy advances, the patient develops decreased sensation to pain or light touch in the radial half of the hand and the first, second, and third digits as well as the radial half of the fourth digit. Thenar muscle atrophy and muscle weakness, especially involving the abductor pollicis brevis, occur in advanced cases of CTS. Positive Tinel and Phalen signs and objective sensory findings in the median nerve distribution confer an 85% diagnostic certainty for CTS. A vast multitude of clinical conditions, ranging from metabolic to traumatic to neoplastic, have been associated with CTS, which can be classified into systemic and local causes. Table 21–1 lists the conditions associated with CTS. In pregnancy, CTS is attributed to fluid retention in the connective tissue due to the hormone relaxin; symptoms are transient and improve after delivery. Local conditions include a wide range of traumatic injuries, infections, tumors, and anatomical variants. Tenosynovitis, burns, or palmar space infections can increase the volume of the carpal tunnel, as do masses such as ganglion cysts, lipomata, xanthomata, neurofibromas, or gouty tophi. Traumatic injuries such as distal radius or carpal bone fractures, or resulting deformities such as unreduced wrist dislocations, or malunion or callus of a Colles fracture, can reduce the capacity of the carpal tunnel. Anomalous muscles or tendons (palmaris profundus, lumbricals, and FDS) and presence of a persistent median artery can lead to mechanical compression of the median nerve. Persistent median arteries occur in 10% of all upper extremities and may compress the median nerve if they are large, thrombosed, or harbor an aneurysm or arteriovenous malformation (AVM). Further important etiologies of CTS include repetitive wrist motion (such as scrubbing, typing, or knitting) that is most often an occupational health issue, and genetic factors, such as a congenitally small carpal canal. The surgeon’s knowledge of these etiological factors should guide the management of CTS. Transient or treatable systemic conditions (i.e., pregnancy or diabetes) can be approached conservatively or medically, and activities involving repetitive wrist motions should be avoided before surgery is undertaken. In over 90% of patients with the clinical diagnosis of CTS, electrodiagnostic studies have been shown to be abnormal. Therefore, nerve conduction studies and electrodiagnostic studies can be highly useful objective measures of diagnostic confirmation. Nerve conduction studies consist of sensory evoked responses, recorded from stimuli applied to the finger via ring electrodes (sensory studies), or from surface electrodes overlying the thenar muscles after electrical stimulation of the nerve (motor studies). They are extremely helpful in localizing the site of compression in median neuropathy, demonstrating conduction block or slowing, which signifies demyelination at the site of compression. The sensory evoked response provides the earliest and most sensitive indicator of CTS: the prolonged distal sensory latency, in which the evoked response can show decreased amplitude or is absent altogether. This sensitive test must be carefully performed and interpreted, for it is influenced by various factors such as age, obesity, edema, and temperature. Comparison studies, in which median nerve conduction is compared with that of another nerve, offer an ideal internal control for these variables. The distal motor latency becomes prolonged in more advanced disease, and a motor latency across the carpal tunnel of greater than 4 msec is considered diagnostic of carpal tunnel syndrome. Electromyography (EMG) is most useful in differentiating CTS from high median neuropathies, C6–C7 radiculopathies, or brachial plexus lesions. EMG studies demonstrate, in the more severe cases, loss of motor units and denervation potentials (fibrillations and positive sharp waves) in the thenar muscles.
 Case Presentation
Case Presentation
 Diagnosis
Diagnosis
 Anatomy
Anatomy
 Characteristic Clinical Presentation
Characteristic Clinical Presentation
 Diagnostic Tests
Diagnostic Tests
| Metabolic/Endocrine | Systemic |
|---|---|
| Diabetes mellitus | Rheumatoid arthritis |
| Hypothyroidism | Amyloidosis |
| Vitamin B6 deficiency | Obesity |
| Acromegaly | Mucolipidoses |
| Renal failure/dialysis | Chondrocalcinosis |
| Gout | Athetoid-dystonic cerebral palsy |
| Pregnancy/lactation | Multiple myeloma |
| Hemophilia | |
| Alcoholism | |
| Sarcoidosis | |
| Traumatic | Anatomical |
| Malunion of Colles/carpal fracture | Persistent medial artery: thrombosed |
| Unreduced dislocation of wrist | Persistent median artery with AVM |
| Compression by cast | Anomalous tendons or muscles |
| Improper immobilization of wrist | Aberrant muscles (palmaris profundus) |
| Burns at wrist | |
| Neoplastic/Mass Lesions | Acquired |
| Ganglion cyst | Repetitive wrist motion |
| Hemangioma | (e.g., typing, knitting, scrubbing) |
| Lipoma | |
| Xanthoma | |
| Neurofibroma | |
| Schwannoma | |
| Infectious | Congenital |
| Septic arthritis | Narrow carpal canal |
| Palmar space infections | |
| Lyme disease | |
| Tuberculosis | |
| Tenosynovitis | |
| Histoplasmosis |
AVM, arteriovenous malformation.
 Management Options
Management Options
Not all patients with CTS require surgical care; indeed, one indication for operative intervention is failure to respond to conservative therapy. Conservative treatment includes splinting, corticosteroid injections into the carpal tunnel, and oral NSAIDs or steroids.
Some patients with a clinical history typical for CTS and confirmatory electrodiagnostic studies may find sufficient relief of previously severe symptoms with conservative therapy alone. However, if the patient continues to experience moderate to severe symptoms despite conservative therapy, operative release of the TCL is indicated. Many surgeons have recognized that CTS is a progressive condition that conservative therapy may temporarily relieve, whereas surgical release offers permanent and effective therapy. Thus other indications for surgery include a history of progressive or unremitting sensory loss, atrophy, or weakness, and a severe median neuropathy with electro-physiological evidence of axonal loss.
Surgical treatment is most effective when offered early in the course of the neuropathy, before significant axonal loss has occurred. A recent retrospective study of 425 patients with CTS demonstrated that patients who had surgery were six times more likely to have resolution of symptoms than were patients who did not have surgery. Furthermore, patients who underwent surgery less than 3 years from the time of initial diagnosis of CTS were more than twice as likely to have symptom resolution than patients who underwent late surgery (more than 3 years after diagnosis). The authors conclude that surgery is a highly effective treatment, but duration of CTS was a key determinant of surgical outcome.
 Surgical Treatment
Surgical Treatment
The TCL release is an established and well-proven therapy for CTS, the goal of which is to adequately divide the TCL while preserving the recurrent motor and palmar cutaneous branches of the median nerve, as well as other neuro-vascular structures. Open release can be done with locally injected anesthesia; our preference is to use 1% lidocaine supplemented with epinephrine.
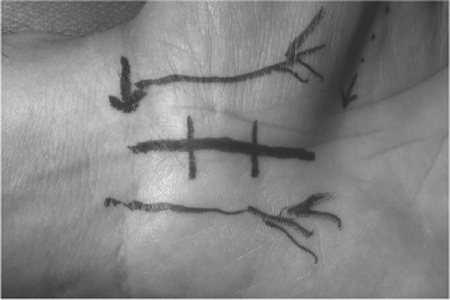
The incision begins at the distal wrist crease at the base of the palm, extending 3 to 4 cm to a point in line with the distal border of the extended thumb. The incision should be placed at the ulnar side of the palmar crease and palmaris longus tendon, in line with the long axis of the ring finger, to avoid the palmar cutaneous branch of the median and ulnar nerves (Fig. 21–1). Beneath the subcutaneous fat, the palmar fascia is found and incised and the TCL exposed; the hypothenar and thenar muscle origins, which may appose in the midline, can at times obscure it. The TCL is divided starting at its midpoint, with a no. 15 scalpel, and has a characteristic gritty, firm consistency. As the TCL is divided in layers the carpal tunnel is entered, exposing its contents of nerve and tendons. With the incision placed as outlined, the surgeon is just typically at the ulnar edge of the nerve. A fine dissector or mosquito forceps is then inserted below the remaining TCL, the median nerve gently dissected away, and the ligament incised sharply using a scalpel or short tenotomy scissors, first distally and then proximally. Distally, the entry into the palmar fat space ensures complete division. Proximally, the remainder of the ligament requires division 2 cm proximal to the wrist crease; the section is extended to the deep fascia of the forearm to completely divide the proximal TCL. The carpal tunnel may then be explored for tumor, ganglion cysts, muscle anomalies, or synovitis. The median nerve itself may appear edematous, flattened, or inflamed (Fig. 21–2) but does not require neurolysis. Once hemostasis has been obtained with bipolar coagulation, the skin is then closed with interrupted vertical mattress nylon sutures, and a bulky hand dressing is applied. Post-operatively, the wrist is not immobilized with a splint and the patient is encouraged to move the fingers through a full range of motion and restrict wrist movement only for a few days until the bandage is removed.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


