Cerebellar Mass
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
Cerebral Ischemia-Infarction, Acute
Hypertensive Intracranial Hemorrhage
Neoplasms
Medulloblastoma (PNET-MB)
Pilocytic Astrocytoma
Hemangioblastoma
Metastases, Parenchymal
Less Common
Enlarged Perivascular Spaces
“Tumefactive” Demyelinating Disease
Multiple Sclerosis
ADEM
Abscess
Cerebellitis, NOS
Vascular Malformation, with/without Hemorrhage
Cavernous Malformation
Arteriovenous Malformation
Dural A-V Fistula
Rare but Important
Tuberculosis
Glioblastoma Multiforme
Dysplastic Cerebellar Gangliocytoma
Oligodendroglioma
Ganglioglioma
Remote Cerebellar Hemorrhage
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Child vs. adult
Child: Neoplasm > infection, demyelinating disease
Adult: Ischemia, hypertensive hemorrhage > neoplasm
Helpful Clues for Common Diagnoses
Cerebral Ischemia-Infarction, Acute
PICA distribution most common
DWI restriction w/correlating ADC map
Early cortical swelling
“Hemorrhagic transformation” in 15-45%
Hypertensive Intracranial Hemorrhage
Round/elliptical high density mass
10% occur in pons, cerebellum
Medulloblastoma (PNET-MB)
4th ventricle > cerebellum
Desmoplastic variant
Pilocytic Astrocytoma
Best clue: Cystic mass + enhancing mural nodule
Childhood (not adult) tumor
Hemangioblastoma
Adult with intra-axial posterior fossa mass with cyst, enhancing mural nodule abutting pia
May be associated with von Hippel-Lindau syndrome
Metastases, Parenchymal
Intra-axial posterior fossa mass in middle-aged/older adult? Think metastasis!
Can be solitary but look for other lesions
Helpful Clues for Less Common Diagnoses
Enlarged Perivascular Spaces
Fluid-filled spaces that look like CSF, surround/accompany penetrating arteries
No diffusion; may have FLAIR hyperintense parenchymal rim
Multiple Sclerosis
Fulminant acute plaque or conglomeration of acute plaques forming mass lesion(s)
May display ring enhancement simulating tumor or abscess
Most common disabling CNS disease of young adults; 1:1000 in developed countries
ADEM
Lesions 10-14 days following infection/vaccination
Large flocculent FLAIR hyperintensity but with less mass effect than that expected
Punctate, ring, incomplete ring, peripheral enhancement
Abscess
Especially in children
Ring-enhancing lesion
High signal on DWI, low ADC
T2 hypointense rim with surrounding edema
Central necrotic area may show presence of acetate, lactate, alanine, succinate, pyruvate, amino acids on MRS
Cerebellitis, NOS
Typically occurs as a primary infectious, post-infectious, post-vaccination, or idiopathic disorder
Variable enhancement → none to intense; meningeal enhancement can be seen
Abnormal T2 hyperintensity & swelling
Bilateral diffuse hemispheric abnormalities are most common (73%)
Cavernous Malformation
“Popcorn ball” appearance with complete hypointense hemosiderin rim on T2WI MR
NECT: 40-60% Ca++
Arteriovenous Malformation
“Bag of black worms” (flow voids) on MR with minimal/no mass effect
Flow-related aneurysm on feeding artery 10-15%; intranidal “aneurysm” > 50%
Dural A-V Fistula
Best imaging tool: DSA with superselective catheterization of feeders
Dural AVF involving the region of the foramen magnum, tentorium, torcula Herophili, or posterior fossa veins (e.g., inferior vermian vein) may affect cerebellum
Most often presents with hemorrhage
Helpful Clues for Rare Diagnoses
Tuberculosis
CECT: “Target sign” → central Ca++ or enhancement surrounded by enhancing rim
T1 C+: Solid homogeneous to rim enhancement; ± central necrosis
MRS: Prominent lipid, lactate but no amino acid resonances
Glioblastoma Multiforme
Thick irregular enhancing rind of neoplastic tissue surrounding necrotic core
Characterized by necrosis and neovascularity
Viable tumor extends far beyond signal abnormalities
Dysplastic Cerebellar Gangliocytoma
Widened cerebellar folia with a striated appearance on MR
Thinning of skull may be apparent
a.k.a., Lhermitte-Duclos disease, associated with Cowden syndrome
Oligodendroglioma
Partially Ca++ subcortical/cortical mass in middle-aged adult
Majority calcify → nodular or clumped Ca++ (70-90%)
May expand, remodel, erode calvarium
Ganglioglioma
Partially cystic, enhancing, cortically based mass in child or young adult
Ca++ common → 35-50%
Cortical dysplasia is commonly associated
Remote Cerebellar Hemorrhage
Occurs after supratentorial craniotomy
Superior cerebellar folia
Bilateral (33%)
Contralateral to side of surgery (29%)
Ipsilateral (22%); isolated vermian (9%)
Image Gallery
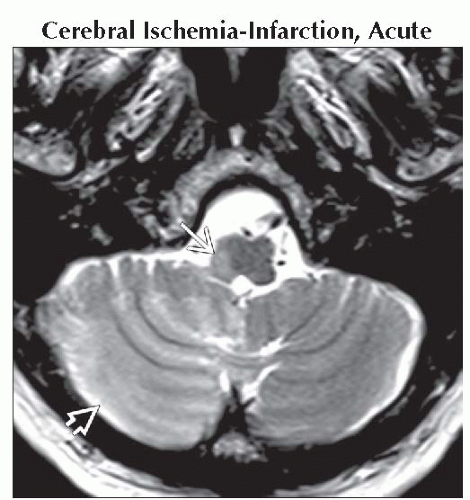 Axial T2WI MR demonstrates a typical case of PICA acute infarction as hyperintensity associated with swelling in the right cerebellar hemisphere  and lateral medulla and lateral medulla  . . |
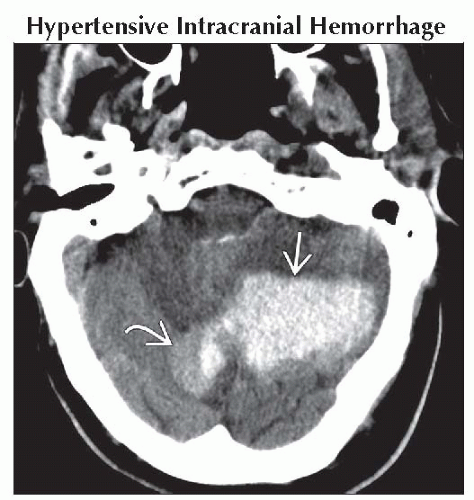 Axial NECT shows a large high density mass in the left cerebellar hemisphere  with some adjacent areas of slightly lesser increased attenuation with some adjacent areas of slightly lesser increased attenuation  , indicating active hemorrhage. , indicating active hemorrhage. |
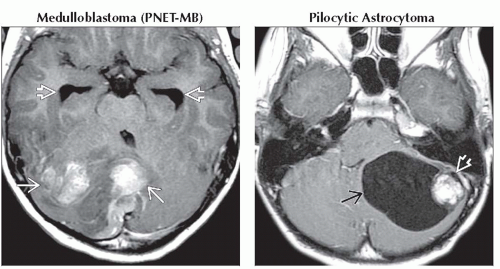 (Left) Axial T1 C+ MR shows a poorly defined mass with components in vermis, right cerebellar hemisphere with irregular pattern of enhancement
 . Note temporal horn enlargement from obstructive hydrocephalus . Note temporal horn enlargement from obstructive hydrocephalus  . (Right) Axial T1 C+ MR shows classic cystic cerebellar pilocytic astrocytoma with nonenhancing rim . (Right) Axial T1 C+ MR shows classic cystic cerebellar pilocytic astrocytoma with nonenhancing rim  , robustly enhancing mural nodule , robustly enhancing mural nodule  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
