Chapter 8 Cervical and Lumbar Sympathetic Blocks
 Sympathetic blocks provide a valuable diagnostic, prognostic, and therapeutic value to sympathetically maintained pain syndromes.
Sympathetic blocks provide a valuable diagnostic, prognostic, and therapeutic value to sympathetically maintained pain syndromes.


 Ultrasound-guided stellate ganglion block may improve the safety of the procedure by direct visualization of vascular structures (inferior thyroidal, cervical, vertebral, and carotid arteries) and soft tissue (thyroid, esophagus, nerve roots).
Ultrasound-guided stellate ganglion block may improve the safety of the procedure by direct visualization of vascular structures (inferior thyroidal, cervical, vertebral, and carotid arteries) and soft tissue (thyroid, esophagus, nerve roots).

 Stellate ganglion block may be associated with serious complications even in experienced hands. Mastering anatomy is of paramount importance.
Stellate ganglion block may be associated with serious complications even in experienced hands. Mastering anatomy is of paramount importance.

Cervical Sympathetic Block
Anatomy
The cervical sympathetic chain is composed of superior, middle, and inferior cervical ganglia. However, in approximately 80% of the population, the inferior cervical ganglion is fused with the first thoracic ganglion, forming the cervicothoracic ganglion, also known as the stellate ganglion (Fig. 8-1).
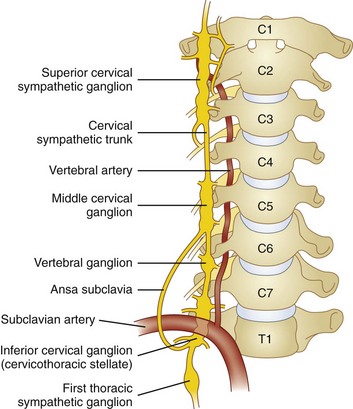
The superior cervical ganglion sends somatic branches via the gray rami communicantes to the cervical plexus (C1-C4), innervating the structures of the neck. The middle and inferior (stellate) ganglia contribute somatic postganglionics to the brachial plexus (C5-T1), innervating the upper extremities.1–3 The superior cervical ganglion sends its vascular branches along the internal and external carotid arteries to reach structures in the cranium, orbit, face, nasal and oral cavities, and pharynx. Blockade of efferents to this ganglion is what results in ptosis, miosis, anhydrosis, and enophthalmos, the classic Horner syndrome. The middle ganglion sends vascular branches along the inferior thyroid artery to the larynx, trachea, and upper esophagus. The inferior (stellate) ganglion sends branches to travel along the subclavian and vertebral arteries. All three cervical ganglia are known to provide visceral branches that contribute to the cardiac plexus. The superior ganglion contributes to the superficial cardiac plexus, and the middle and inferior ganglia contribute to the deep cardiac plexus.
Most preganglionic sympathetic efferents innervating the head, neck, and upper extremity either pass through or synapse at the stellate ganglion. This provides us with an ideal target for blockade of sympathetic efferents to the head, neck, and upper limbs. Occasionally, additional sympathetic innervation to the upper extremity exits the sympathetic chain via gray rami communicantes at T2 and T3 and goes on to the distal upper extremity without ever passing through the stellate ganglion.4,5 The prevalence of this anomaly is unknown but should be kept in mind when interpreting the results of the block because it could result in failed sympathetic denervation despite adequate blockade of the stellate ganglion.
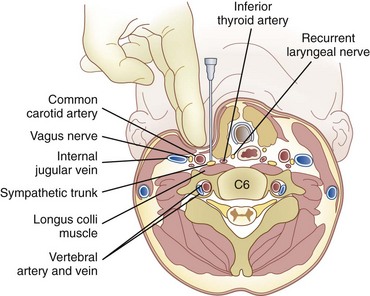
The stellate ganglion is located medial to the scalene muscles; lateral to the longus colli muscle, esophagus, and trachea along with the recurrent laryngeal nerve (RLN); anterior to the transverse processes and prevertebral fascia; superior to the subclavian artery and the posterior aspect of the pleura; and posterior to the vertebral vessels at the C7 level.6 This explains why there may be increased risk of pneumothorax and vertebral artery injury with blockade at the C7 level.
The stellate ganglion measures approximately 2.5 cm long, 1 cm wide, and 0.5 cm thick (anteroposterior [AP] diameter). It is usually located posteriorly in the chest in front of the neck of the first rib and may extend to the seventh cervical (C7) vertebral body.6–8 If the inferior cervical ganglion and first thoracic ganglion are not fused, the inferior cervical ganglion lies in front of the C7 tubercle, and the first thoracic ganglion rests over the neck of the first rib.6–8 Accordingly, by using the blind technique at C6, the ganglion primarily blocked is the middle cervical ganglion, and the cervicothoracic ganglion is blocked if the injectate spreads down to the T1 level.
Indications
Other less commonly encountered indications include hyperhidrosis, Ménière disease, accidental intraarterial injection of intravenous medications, and angina pectoris.9 More recently, stellate ganglion block has been used for the treatment of patients with hot flashes and posttraumatic stress disorders.10,11
Technique
C6 Anterior Approach
The stellate ganglion block is most commonly performed with an anterior approach at C6 transverse process (Chassaignac tubercle).12–14 The anatomical landmarks allow this block to be performed either with or without fluoroscopic guidance.
The patient is placed in the supine position with support under the shoulders and the head resting flat on the table. This position provides slight extension of the neck and facilitates palpation of the necessary anatomical landmarks. The C6 transverse process can be easily located by first palpating the cricoid cartilage. Chassaignac tubercle is located between the cricoid cartilage and the medial border of the sternocleidomastoid. With the index and middle fingers of the nondominant hand, pressure is applied to compress the subcutaneous tissues and identify the C6 transverse process. The pulsations of the carotid artery should be palpated, and an attempt should be made to retract the carotid artery laterally to keep it out of the path of the needle (Fig. 8-2). The cranial and caudal borders of the transverse process are identified with the index and middle fingers, and the block needle is inserted directly between the two fingers to ensure contact with bone.
After negative gentle aspiration, an initial test dose of 0.5 to 1.0 mL of local anesthetic should be injected. Intravascular injection of less than 1 mL of local anesthetic has been reported to cause loss of consciousness and seizure activity.15 If no signs or symptoms of intravascular injection have been observed, a solution of 5 to 10 mL may be injected with re-aspiration after every 3 to 5 mL to help ensure persistent extravascular needle placement.
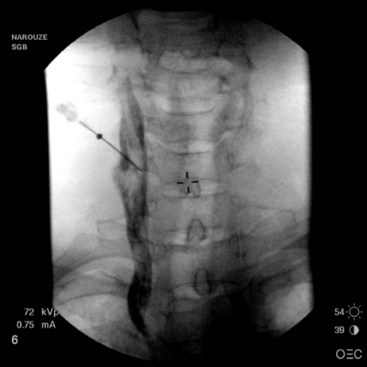
If using fluoroscopy for the procedure, injection of 1 to 2 mL of nonionic contrast should be injected before injection of local anesthetic. It should be visualized traveling inferiorly with minimal resistance. If the needle tip has been placed medially along the transverse process, contrast spread my have a striated appearance, indicating tip placement within the longus colli muscle (Fig. 8-3). If this is the case, the needle should be withdrawn slightly and contrast reinjected to demonstrate the characteristic “honeycomb” appearance indicating that the needle tip is in the appropriate fascial plane anterior to the muscle (Fig. 8-4). Real-time fluoroscopy should be used for careful assessment of any sign of intravascular injection.


C7 Anterior Approach
The stellate ganglion block can also be performed at C7.16 The approach is nearly identical to the C6 approach; however, the anatomical landmarks are more difficult to identify because the C7 vertebra has only a vestigial tubercle that is not readily palpable. Hence, the procedure is usually performed with fluoroscopy. When performing the block without fluoroscopic guidance, it is easier to first palpate the C6 tubercle and then move one fingerbreadth inferior as an estimate of the C7 tubercle. At this level, the risk of pneumothorax and vertebral artery injury is higher.17
An oblique fluoroscopic approach18 targeting the junction between the uncinate process and the vertebral body at the C7 level was described in an effort to decrease those risks.
The C7 approach does offer a few advantages, however. Because the needle is closer in proximity to the stellate ganglion, which resides directly anterior to the C7 transverse process, a smaller volume of solution can be injected to produce a more reliable and consistent blockade.19 This may be of particular value when the patient has failed previous block at the C6 level.
Limitations and Evolution of Current Techniques
Because the stellate ganglion is located in close proximity to various critical structures, its blockade may be associated with a number of complications, some of which are life threatening. Accordingly, techniques for blockade have evolved and varied from the use of the standard blind technique to the use of radionuclide tracers,20 computed tomography,21 and magnetic resonance imaging.6,22 However, these techniques are not practical in daily clinical practice because they are time consuming, cost-ineffective, and involve radiation exposure. Fluoroscopy has been suggested as a safer and more effective way to perform stellate ganglion block than the traditional blind approach.18,23
Vascular structures (inferior thyroidal, cervical, vertebral, and carotid arteries) and soft tissue (thyroid, esophagus, nerve roots) are also not seen with fluoroscopy—contrary to with ultrasonography—and are therefore at risk of injury with fluoroscopy-guided techniques.24
Ultrasound-guided stellate ganglion block may improve the safety of the procedure by direct visualization of the related anatomical structures, and accordingly the risk of vascular and soft tissue injury may be minimized. Also, ultrasound guidance allows direct monitoring of the spread of the injectate, so complications such as RLN palsy, intrathecal, epidural, or intravascular spread may be minimized as well. The absence of the spread of local anesthetic during the real-time injection raises the suspicion of intravascular injection.25
Ultrasound-Guided Cervical Sympathetic Block
Kapral et al26 first described ultrasound imaging for stellate ganglion block. In their case series, 12 patients received the classical “blind” stellate ganglion block followed by ultrasound-guided block the next day. The blind technique resulted in “asymptomatic” hematoma formation in three of 12 patients, with no hematoma occurring with the ultrasound technique. The spread of the local anesthetic was observed under real-time sonography, and the proximity of the local anesthetic to the RLN and nerve root correlated well with complications such as hoarseness and paresthesia. In this study, 5 mL of local anesthetic was administered, and all patients in the ultrasound-guided group developed sympathetic block compared with 10 out of 12 in the blind group.
Shibata et al27 noted more caudad injectate distribution and better sympathetic blockade with less incidence of hoarseness with ultrasound-guided subfascial injection compared with suprafascial injection.25 Contrary to the fluoroscopy-guided method, the end point of the needle is not the contact with bone but the prevertebral fascia.24,27
With injection anterior to the prevertebral fascia, the solution tends to spread around the carotid sheath (Fig. 8-5).28 In this case, the risk of hoarseness is higher, probably secondary to proximity of the vagus nerve in the carotid sheath and the RLN medial to the carotid and lateral to the trachea.27,28

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


