Chapter 94 Cervical Facet Dislocations
A Ventral Surgical Strategy for Decompression, Reduction, and Stabilization
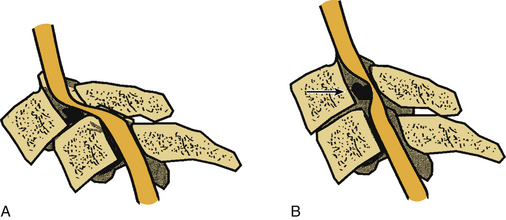
Much controversy surrounds the management of subaxial cervical subluxations resulting from facet fracture-dislocation.1–11 An initial attempt at closed reduction using skeletal traction is not without risk.12–18 The most serious complication of cervical traction and closed reduction is the retropulsion of disc fragments into the spinal canal and resultant spinal cord compression (Fig. 94-1). Several reports of neurologic deterioration after closed reduction in the setting of concurrent disc herniation have been described.19–23 In addition, late instability is relatively common in patients treated with closed reduction alone, because of the concomitant presence of significant ligamentous disruption associated with these injuries.
The surgical technique for the open reduction of unstable cervical dislocations varies from surgeon to surgeon. Most reports have described dorsal reduction techniques.20,21,24–29 However, the ventral surgical approach for reduction has its advocates.30 Several small series have been published that describe the technique of ventral reduction of locked facets.19,31–35 Because of the popularization of dorsal fixation techniques (e.g., lateral mass plating and spinous process wiring), ventral reduction has not been widely used in clinical practice. However, an increasing concern has been raised regarding the danger associated with the dorsal reduction of a cervical spine dislocation in the presence of a ventral disc herniation.19,21–24 Furthermore, because of the common coexistence of significant dorsal bony and soft tissue disruption, a three-vertebral segment (two-motion segment) dorsal fixation is commonly required to stabilize a two-vertebral segment (one-motion segment) instability. In addition, in dorsal reduction of locked facets, it is commonly necessary to remove a significant portion of the involved facet(s), thus often mandating a three-vertebral segment dorsal fixation procedure. Conversely, ventral reduction may be followed by arthrodesis of only a single-motion segment, thus sparing additional motion segments from arthrodesis.
Kwon et al.36 concluded that both ventral stabilization and dorsal stabilization for unilateral cervical facet injuries were valid treatment options. In this randomized study of 42 patients with unilateral cervical facet injuries, patients on whom a ventral approach was used had a lower rate of wound infection, had a higher rate of radiographically demonstrated union, and healed in a more lordotic sagittal alignment. However, they also more frequently had signs of dysphagia and voice changes in the early postoperative period in comparison to the group treated with dorsal stabilization. Patients undergoing a ventral approach should be informed of these (and all other) risks.
Surgical Technique
Discectomy
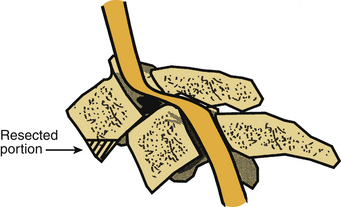
The standard ventromedial approach is used through a transverse skin incision. After radiographic confirmation of the operative level, a discectomy is performed. A special consideration in the case of facet dislocation is the ventral translation (ventrolisthesis) of the rostral vertebral body on its caudal counterpart. This is often associated with some degree of kyphotic angulation and a resultant obscuration of the disc space, necessitating removal of the ventral aspect of the caudal end plate of the rostral vertebral body with a high-speed air drill (Fig. 94-2). Care must be taken not to remove so much of the vertebral body as to preclude ventral screw-plate fixation. After exposure of the disc space, a standard discectomy is performed. The posterior longitudinal ligament is always removed, thus exposing the dura mater and ensuring adequate decompression.
Reduction
Interbody Spreader Technique
A Cloward interbody spreader, or an equivalent device, is inserted into the disc interspace at a 30- to 40-degree angle (Fig. 94-3A). Failure to place this device at an angle results in achieving only distraction force application (as simple distraction with tongs achieves). This does not result in the application of a bending moment, which is required for reduction with this technique.
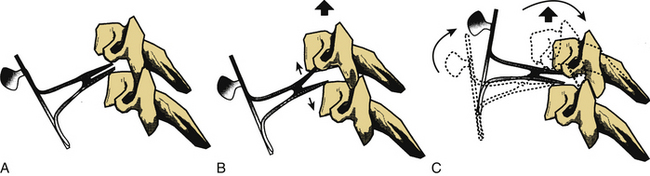
While distraction is gradually applied with the disc interspace spreader (applied in the midvertebral body region) (Fig. 94-3B), the spreader is rotated rostrally. This applies a bending moment to the dislocated vertebral body while the facet dislocation is reduced by distraction. If the locked facets are disengaged, the vertebrae should realign. Distraction is then relaxed in the aligned position, and the spreader is removed (Fig. 94-3C).
Vertebral Body Post Technique
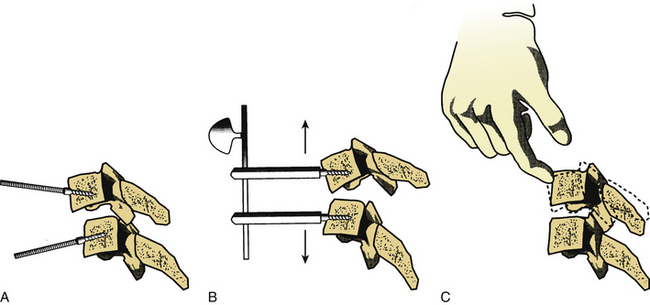
The vertebral body post technique usually involves placing the posts at an angle with respect to each other (Fig. 94-4A). This facilitates the application of a bending moment that unlocks the facets before the application of distraction forces (Fig. 94-4B). Distraction should then allow for complete disengagement of the locked facets. Manual reduction via the placement of the dorsally directed pressure on the rostral vertebral body encourages reduction if the facets have been adequately disengaged (Fig. 94-4C). Relaxation of the distraction forces then allows reengagement of the facets in a normal position. The placement of dorsally directed pressure on the rostral vertebral body, as described previously, may also be applied with the interbody spreader technique.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


