Cervical Spine Kinematics and Clinical Instability
Cervical Spine Kinematics and Clinical Instability
Paul C. Ivancic
Jiří Dvořák
Vijay K. Goel
Todd A. Fairchild
Augustus A. White III
Denis J. DiAngelo
With the advent of novel methods of evaluating both normal and abnormal motions of the cervical spine, a more complete understanding of cervical spine stability continues to evolve and be defined. This more cogent definition, in turn, may directly assist the clinician in the often daunting task of evaluating the clinical stability of the cervical spine. The goals of this chapter are to introduce the biomechanical concept of kinematics or the study of motion of the spine, to define the role of anatomical elements in providing mechanical stability to the spine, and to provide some practical guidelines for determining clinical instability.
BASIC CONCEPTS
Kinematics is the study of the motion of bodies without consideration of the influencing forces. The challenge for the clinician is to become familiar with the normal spinal range of motion (ROM) and the characteristic patterns of motion. The ranges are generally expressed as rotation and translation in three planes. Excessive motion may be indicative of structural spinal damage. Too little motion may accompany stiffness and pain. There may also be irregularity in the pattern of motion. Abnormal motion patterns that have been described include irregular scatter of the instantaneous axes of rotation (IARs), reversed coupling patterns, and rotation of vertebra in uncharacteristic directions. The study of kinematics provides a basis for determining when excessive or irregular motion may be associated with pain or neurologic impairment. The following metaphor from Lovett’s classic work (1) on the mechanism of the normal spine and its relation to scoliosis serves as an excellent introduction to a presentation of the normal kinematics of the cervical spine:
It is as if one undertook, for example, to investigate a railroad accident solely from a study of the wrecked cars. Much could be learned as to the effect and direction of the destructive forces, the amount of force expended, and the kind of damage done, but more could be learned and future accidents could be better prevented by a study of the normal running of the trains and their proper relations to each other at the time of the accident and by an investigation of the signal system and the routine precautions adopted.
The key to the “normal running of the trains” is the kinematics of the spine. With a thorough knowledge of kinematics, the clinician is more likely to make new discoveries of irregularities and correlate them with clinical conditions. A thorough knowledge of spinal kinematics is helpful in understanding all aspects of the diagnosis and management of spinal pathology and is especially true of the cervical spine, for it is the most mobile region of the spine.
PHYSIOLOGIC MOTION AND FUNCTIONS OF THE CERVICAL SPINE
To analyze, understand, and correct the various malfunctions of the spine, it is essential that we first fully characterize the normal functions. The three functions of the human spine are to (a) support the appendicular skeleton and the trunk, (b) protect the neural elements, and (c) allow a significant amount of complex motion. Certain clinical problems are known to be associated with irregularities in the amount and possibly the type of motion present in the spine. Some of the diseases associated with irregular motion in the spine are well recognized and documented through clinical observations. Other diseases may be associated with motion irregularities even though the full pathology and associated clinical consequences have not yet been fully characterized.
The functions and anatomic designs of the occipitoatlantoaxial complex (C0-C1-C2) and the lower cervical spine (C2 through C7) are dissimilar; therefore, it is advantageous to study the kinematics of each region separately. The occipitoatlantoaxial complex is grouped and labeled the upper cervical spine. Because of kinematic (2), kinetic (3), and clinical uniqueness (4,5), the cervical region is further divided into the middle cervical (C3 through C5) and the lower cervical (C6 through T1) regions.
RELEVANT BIOMECHANICAL TERMS AND TESTING METHODS
Some key kinematic terms are defined herein to facilitate further reading (6).
Translation: Translation is motion of a rigid body in which a straight line in the body always remains parallel to itself.
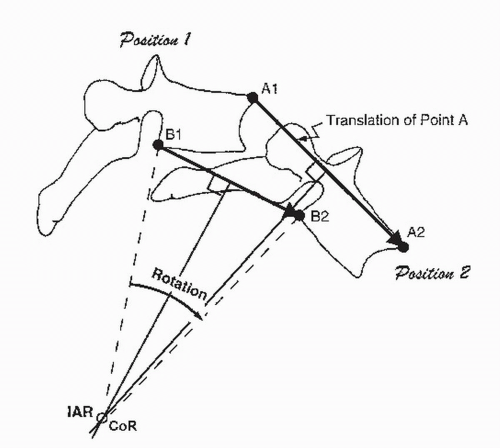
Rotation: Rotation is motion of a rigid body in which a straight line does not remain parallel to itself (Fig. 4.1). The angle between the two positions of the straight line, that is, A1-B1 and A2-B2, is the angle of rotation.
Center of Rotation (COR): When a rigid body moves in a plane, there is a point, either in the body or at some hypothetical extension of it, that does not move. This is the COR of the body for that step of motion (see Fig. 4.1). The line perpendicular to the motion plane and passing through the COR is called the IAR. The COR or IAR is obtained by the intersection of the perpendicular bisector of the translation vectors A1-A2 and B1-B2 of any two points, for example, points A and B.
Degrees of Freedom (DOF): The number of independent coordinates in a coordinate system required to completely specify the position of an object in space.
Neutral Position: The erect posture of the spine in which the overall internal stresses in the spinal column and the muscular effort to hold the posture are minimal.
Range of Motion: The range of physiologic intervertebral motion measured from the neutral position. It is divided into two parts: neutral zone (NZ) and elastic zone (EZ).
Neutral Zone: That part of the range of physiologic intervertebral motion, measured from the neutral position, within which the spinal motion is produced with a minimal internal resistance. It is the zone of relatively high flexibility or laxity.
Elastic Zone: That part of the range of physiologic intervertebral motion measured from the end of the NZ up to the physiologic limit. In the EZ, spinal motion is produced against a significant internal resistance. It is the zone of high stiffness.
Figure 4.1. A vertebra is shown in two positions in the sagittal plane. The motion is rotation about the COR or about the IAR.
BIOMECHANICAL TESTS
In vitro biomechanical tests include strength, fatigue, or flexibility (7). A strength test consists of applying a load to an implant or a spinal construct (specimen plus instrumentation) until it fails and determining its load carrying capacity. A fatigue test determines the capacity of the spinal construct to carry varying physiologic loads until the fusion matures and unloads the implant. The load can be varied but is always less than the failure load. The cyclic load is applied until the specimen fails. A stability test determines the capability of the spinal construct to minimize motion at the site of fusion to promote initiation of fusion and maturation. Stability testing can be further divided into flexibility and stiffness testing. To conduct a stability test, the specimen is subjected to load (force or moment) or displacement (translation or rotation). Flexibility testing consists of applying loads and measuring resulting displacements, while stiffness testing consists of applying displacements and measuring resulting loads.
IN VIVO KINEMATICS
The concept of in vivo passive kinematics has been well described in the work of Dvorak et al. (8, 9 and 10). Investigations with functional x-rays have showed that additional motion can be gained by exerting external forces on the “fully” flexed or extended neck, an important finding to consider when evaluating voluntary flexion/extension tests. This is also consistent with the assertion that the stretch test (passive axial traction) is more likely to show existing pathology than is measurement of active (i.e., voluntary) flexion/extension (6).
The differences between active and passive in vivo ROM must be considered in the interpretation of laboratory and clinical studies of normal ranges of cervical motion. Considering that in daily clinical routine we do not deal with healthy volunteers but rather with patients who have either injury or painful conditions resulting from ongoing degenerative changes, we must be aware that the patient’s active motion may be restricted by motion-induced pain rather than pathology (11, 12 and 13). However, we should be concerned, especially when we suspect a segmental instability, in motion (both rotation and translation) beyond the limit of active motion. In an injured patient population, examination of passive flexion/extension was shown to result in the identification of more hypermobile segments (9,14). Similar observations as related to passive motion of the cervical spine have been made with lateral bending (15) and axial rotation (10). Examining the total motion of the cervical spine with a spine motion analyzer (16), it was found that passive tests resulted in larger ROM with smaller associated standard deviation (SD). Active tests showed significantly less motion than passive tests in measurements of lateral bending and axial rotation of the cervical spine. A meta-analysis of average cervical spine motion (17) of healthy individuals between 20 and 50 years of age found increased passive motion, as compared to active (140 vs. 126 degrees total flexion/extension; 109 vs. 86 degrees total lateral bending; 174 vs. 151 degrees total axial rotation).
AN ONGOING FIELD
Much of the research presented herein requires further confirmation and suggests new avenues for investigation. Attempts have been made to distill fact from postulate and to integrate biomechanical research with clinical applications. As in any research field, there are numerous problems to overcome. The kinematics of interest is that of the in vivo cervical spine. The experimental techniques for precise, no-risk, in vivo measurements continue to evolve. The characteristics of the muscle forces that result in in vivo physiologic motions have recently been emulated during experimental motion testing (18). In vitro studies have been performed to simulate vertebral motion, but whether the motions produced experimentally are the same as those produced in vivo is not known. Obviously, these problems must be addressed. The purpose of this chapter is to present the state of the art in regard to cervical spine kinematics; useful areas of clinical relevance are indicated.
BASIC CERVICAL SPINE KINEMATICS
The measurement of cervical spine motion is a routine part of the clinical examination of patients with neck pain resulting from either injury or degenerative changes. Methods of recording motion data, including goniometry, functional radiography, or visual estimation, have varying accuracy and repeatability (4,19, 20, 21 and 22). The understanding and knowledge of normal neck ROM based upon age, gender, and neck size forms the basis for analysis of altered and possibly pathologic motion patterns as well as increased or decreased ROM (16,20,23,24).
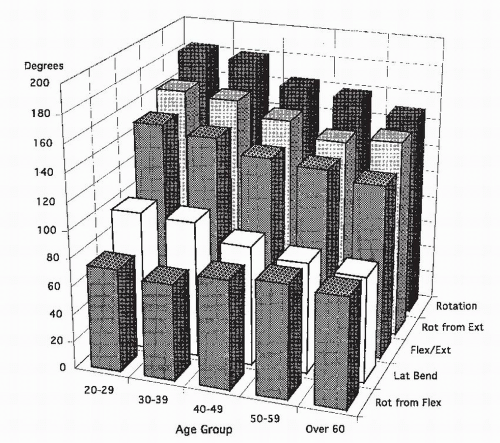
Figure 4.2. With increased age, there is an overall decrease in motion due to the normal agerelated changes in the cervical spine. In one study (16), the largest decrease in motion occurred in the age groups of 30 to 39 and 40 to 49 years. Rotation from flexion (axial rotation with cervical spine in full flexion) is the only motion that stayed the same or actually increased slightly with age. (Reprinted from Dvorak J, Antinnes JA, Panjabi MM, et al. Age and gender related normal motion of the cervical spine. Spine 1992;17:S393-S398, with permission.)
To obtain normal values, 150 healthy, asymptomatic volunteers were tested (CA-6000 Orthopedics Systems, Hayward, CA) (16). The subject was seated in a specially designed chair, and the device attached and zeroed. Active, followed by passive, ROM measurements were collected for flexion/extension, axial rotation, lateral bending, and rotation out of maximum flexion and extension.
The volunteers were divided into groups based on gender and the following age decades: 20 to 29, 30 to 39, 40 to 49, 50 to 59, and 60+ years. The overall tendency was for ROM to decrease as age increased (Fig. 4.2). This proved true in nearly all motions, with the most dramatic decrease in motion occurring between the groups aged 30 to 39 and 40 to 49 years. The only motion that did not decrease with age was the rotation out of maximum flexion, which remained the same or showed a slight increase, on average, as age increased. The average values for age decades for each motion as well as average for the gender groups along with significant differences are shown in Table 4.1. Significantly less motion in the active tests was evident in comparison of lateral bending and axial rotation. Generally, for passive tests, the SD was lower (Table 4.2).
TABLE 4.1 Average (SD) Head-Shoulder Rotations in Degrees
a Significant difference from cell directly adjacent to the right (i.e., gender within age group differences).
b Significant difference from cell directly adjacent below (i.e., age group within gender differentiation).
Women showed greater ROM than men. In the age range of 40 to 49 years, women again showed significantly greater ROM in axial rotation and rotation at maximal flexion. There were no significant differences between gender groups for the group aged 60+ years. The wellestablished clinical observation that motion of the cervical spine decreases with age (17,25,26) has been confirmed in this study (16). An exception to this finding was the surprising observation that the rotation of the upper cervical spine, mainly at the atlantoaxial joint (tested by rotating the head at maximum flexion of the cervical spine that presumably locks the other levels) did not decrease with age. The measurement data for rotation out of maximum flexion suggests that the rotation of the atlantoaxial joint does not decrease with age, but rather remains constant or increases slightly perhaps to compensate for the reduced motion of the lower segments.
Tommasi et al. (27) used an optoelectronic motiontracking system to evaluate active three-dimensional (3-D) neck ROM in healthy female volunteers in three age groups: 15 to 18, 20 to 30, and 35 to 45 years. They generally found decreases in ROM with increasing age, with the exception of axial rotation. The greatest decrease of 10 degrees was observed in flexion/extension followed by 3 degrees in lateral bending. In a study of asymptomatic volunteers in seven age groups, 20 to 29 through +80 years, Lansade and associates (28) investigated the effects of age and gender on active main and coupled neck motions and proprioception using an infrared motion-tracking system. With increased age, they observed significant reduction in proprioception and in main ROM, between 0.6 and 0.8 degrees per decade.
TABLE 4.2 Comparison of Means and Degrees for Normal Active Cervical Spine Rotations
In a clinical study, Mayer et al. (20) used two inclinometers connected to a computer system to measure flexion/extension, lateral bending, and axial rotation. Fifty-eight normal subjects (mean age 32 years) were divided into two groups: the 50% youngest versus the 50% oldest. Using this kind of division of the normal group, the investigators noted no gender- or age-related differences in ROM possibly due to the small groups and/or the mean age of the group (32 years, SD = 12.6 years). Comparison with the study by Dvorak et al. (16) showed the dramatic decrease in ROM occurs between the fourth and fifth decades of life, a finding also demonstrated in the pathologic and anatomic studies of Luschka (29) and later confirmed by Töndury and Theiler (30).
Three-dimensional neck motions were continuously measured during activities of daily living over a 5-day period in healthy young adults (31,32). Results indicated that most neck motions were less than 15 degrees, with flexion-extension occurring twice as frequently as axial rotation and lateral bending. These results may be useful to clinicians when determining treatment modalities based upon the underlying injury or pathology and to engineers for designing motion-preserving spinal implants.
UPPER CERVICAL SPINE: C0-C1-C2
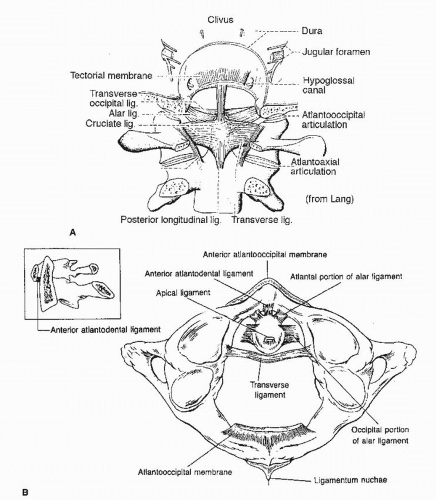
Most of the axial rotation and some of the flexion-extension and lateral bending of the head occur in the upper cervical spine. The highly specialized anatomy of this region is designed to provide seemingly paradoxical attributes: flexible enough to allow nearly 50% of the cervical spine axial rotation, sufficiently stiff to protect delicate structures of the spinal cord and vertebral arteries, and strong enough to carry the weight of the head and resist muscle forces. It is therefore a very complicated structure, with motion determined by the orientation of the articular processes and limited by the ligaments (Fig 4.3).
The atlantooccipital (C0-C1) joints are spheroid articulations; that is, they allow motion in the shape of a sphere. The joint capsule connecting them is very tight, serving to limit the possible movements and prevent dangerous hypermotion that could pinch the spinal cord or the vertebral arteries. The dominant movement in the atlantooccipital joint is flexion and extension of approximately 24 degrees (Table 4.3). The lateral bending is 5 to 10 degrees. The idea of axial rotation in this joint has long been rejected but, more recently, investigators have shown axial rotation in both in vitro and in vivo studies (33, 34, 35 and 36). The possible movements in the atlantooccipital joint are shown in Table 4.3. The disparity in the results is mostly due to the differences in the methods used in the mixed group of in vitro and in vivo studies.
Figure 4.3. A: Ligaments of the upper cervical spine, dorsal view. (Reprinted from Lang J. Kleinische Anatomie aer Halswirbelsäule. Stuttgart: G. Theme Verlag, 1991, with permission.) B: Top view of the C1-C2 joint. Schematic of the major ligaments involved in the clinical stability of the upper cervical spine.
TABLE 4.3 Average Rotations in Degrees at the Atlantooccipital Joint (C0-C1)
The disparity in the results is most likely due to the differences in the methods used in the mixed group of in vitro and in vivo studies.
The atlantoaxial (C1-C2) joint consists of four joint spaces: the two atlantoaxial lateral joints, the atlantoaxial median joint (between the ventral arch of the atlas and the dens axis), and a joint between the dorsal surface of the dens and the transverse ligament, which is connected to the ventral joint space. From the medial part, there is a large synovial fold in the lateral atlantoaxial joint. This joint capsule, in contrast to that of the atlantooccipital joint, is loose, allowing a great deal of motion. It is here that most of the axial rotation occurs, a fact reflected in the anatomy as the vertical dens of the axis (C2) acts as a pivot about which the atlas (C1) rotates. The possible movements in the atlantoaxial joint are summarized in Table 4.4. As in Table 4.3, the differences in the results of the studies are due to the different methods used.
The motion in the upper cervical spine, especially in the atlantoaxial joint, is mainly limited by the nonstretchable collagen fibers (37) of the alar ligaments, which connect the dens to the medial aspects of the occipital condyles and ventral arch and lateral masses of the atlas (34,38). According to Werne (39), alar ligaments are of great importance in limiting axial rotation—a belief that has been confirmed by newer investigations (Fig. 4.4) (34,40). In conjunction with the tectorial membrane (the only elastic ligament in the upper cervical spine), the alar ligaments also limit the flexion of the occiput. During lateral bending (Fig. 4.5), the alar ligament is responsible for forced axial rotation of the second vertebra in the same direction as the lateral bending (10,39). The spinous process of the axis moves contralaterally.
TABLE 4.4 Average Rotations in Degrees at the Atlantoaxial Joint (C1-C2)
As in Table 4.3, the differences in the results are due to the different methods used.
The cruciate ligament (Fig. 4.3A and B) has cleverly evolved to restrict potentially dangerous ventral motion of the atlas during flexion movement of the head while still allowing the atlas to turn freely around the dens during axial rotation. It consists of two main parts: the horizontally oriented transverse ligament and the vertically oriented longitudinal fibers. At the level of the dens, there is a thin layer of cartilage covering the transverse ligament (8), which allows the ligament to move more freely during rotation and protects it from friction damage. The transverse ligament consists of collagen fibers with an interesting fiber orientation similar to a folding lattice. This allows extensive stretching of the ligament during axial rotation without damage to the fibers. In vitro experiments indicate failure of the transverse ligament at a wide range of loads, between 118 and 1,765 N (8,41,42). The apical ligament has no functional meaning.
Only gold members can continue reading. Log In or Register to continue