Disorders of Speech and Language: Introduction
Speech and language functions are of fundamental human significance, both in social interaction and in private intellectual life. When they are disturbed as a consequence of brain disease, the functional loss exceeds in many ways all others in gravity—even blindness, deafness, and paralysis. The neurologist is concerned with all derangements of speech and language, including those of reading and writing because they are almost invariably manifestations of disease of the brain.
Viewed broadly, language is the means of symbolic representation of objects, actions, and events and, therefore, the mirror of all higher mental activity. The internal manipulation of these symbols constitutes thinking and their retention is the substance of memory. In a narrower context, language is the means whereby patients communicate their complaints and problems to the physician and at the same time, the medium for all delicate interpersonal transactions. Consequently, any disease process that interferes with speech or the understanding of spoken words touches the very core of the physician–patient relationship. Finally, the study of language disorders and the development of language (taken up in Chap. 28) serve to illuminate the relationship between psychologic functions and the anatomy and physiology of the brain.
General Considerations
It has been remarked that as human beings, we owe our commanding position in the animal world to two faculties: First, the ability to develop and employ verbal symbols as a background for our own ideation and as a means of transmitting thoughts, by spoken and written word, and second, the remarkable facility in the use of our hands. One curious and provocative fact is that both language and manual dexterity (as well as praxis) have evolved in relation to particular aggregates of neurons and pathways in one cerebral hemisphere (the dominant one). This is a departure from most other localized neurophysiologic activities, which are organized according to a contralateral or bilateral and symmetrical plan. The dominance of one hemisphere, usually the left, emerges in brain development together with speech and the preference for the right hand, especially its use for writing. It follows that a lack of development or loss of cerebral dominance as a result of disease deranges both these traits, causing aphasia and apraxia.
There is abundant evidence that higher animals are able to communicate with one another by vocalization and gesture. However, the content of their communication is their feeling or reaction of the moment. This emotional language, as it is called, was studied by Charles Darwin, who noted that it undergoes increasing differentiation in the animal kingdom. Only in the chimpanzee do the first semblances of propositional language become recognizable. Indeed, there are distinct differences between the human and chimp versions of a gene called FOXP2, which has been linked to the ability to produce language, as noted in Chap. 28 (also see Balter). Another genetic influence on language has been found by Somerville and colleagues, who studied the locus implicated by a deletion in Williams syndrome and found that a duplication at this site caused a severe delay in the acquisition of expressive speech (see Chap. 38 for a discussion of the skills that are affected in Williams syndrome).
Instinctive patterns of emotional expression are, of course, also observed in human beings. They are the earliest modes of expression to appear (in infancy) and may have been the original forms of speech in primitive human beings. Moreover, the utterances we use to express joy, anger, and fear are retained even after destruction of all the language areas in the dominant cerebral hemisphere. The neural arrangement for this paralinguistic form of communication (intonation, exclamations, facial expressions, eye movements, body gestures), which subserves emotional expression, is bilateral and symmetrical and does not depend solely on the cerebrum. The experiments of Cannon and Bard demonstrated that emotional expression is possible in animals even after removal of both cerebral hemispheres provided that the diencephalon, particularly its hypothalamic part, remains intact. In the human infant, emotional expression is well developed at a time when much of the cerebrum is still immature.
Propositional, or symbolic language differs from emotional language in several ways. Instead of communicating feelings, it is the means of transferring ideas from one person to another, and it requires the substitution of a series of sounds or marks for objects, persons, and concepts. This is the essence of language. It is not instinctive but learned and is therefore subject to all the modifying social and cultural influences of the environment. However, the learning process becomes possible only after the nervous system has attained a certain degree of maturation. Mature language function involves the comprehension, formulation, and transmission of ideas and feelings by the use of conventionalized verbal symbols, sounds, and gestures and their sequential ordering according to accepted rules of grammar. Facility in symbolic language, which is acquired over a period of 15 to 20 years, depends on maturation of the nervous system and on education. Many attempts have been made to crystallize the essential difference between human language and that of the higher primates that are able to communicate. Such distinctions, of course, bear on the definitions of language-dependent function, such as thinking, analysis, synthesis, and creativity. Beyond simply the complexity and range of symbolic representation and grammar available to humans in comparison to animals, Chomsky has proposed that the ability to frame recursive ideas (ones that refer to themselves by embedded phrases, such as: “John’s sister’s house”) underlies creativity in human language and an infinite variety of sentences. This has been challenged but is an interesting concept.
Although speech and language are closely interwoven functions, they are not synonymous. Language refers to the production and comprehension of words whereas speech refers to the articulatory and phonetic aspects of verbal expression. A derangement of language function is always a reflection of an abnormality of the brain and, more specifically of the dominant cerebral hemisphere. A disorder of speech may have a similar origin, but not necessarily; it may be a result of abnormalities in different parts of the brain or to extracerebral mechanisms.
The profound importance of language may not be fully appreciated unless one reflects on the proportion of our time devoted to purely verbal pursuits. External speech, or exophasia, by which is meant the expression of thought by spoken or written words and the comprehension of the spoken or written words of others, is an almost continuous activity when human beings gather together. This contrasts with inner speech, or endophasia, i.e., the silent processes of thought and the formulation in our minds of unuttered words on which thought depends. The latter is almost incessant during our preoccupations, as we think always with words. Thought and language are thus inseparable. In learning to think, the child talks aloud to himself and only later learns to suppress the vocalization. Even adults may mutter subconsciously when pondering a difficult proposition. As Gardiner has remarked, any abstract thought can be held in mind only by the words or mathematic symbols denoting it. It is virtually impossible to comprehend what is meant by the word religion, for example, without the controlling and limiting consciousness of the word itself. “Words have thus become an integral part of the mechanism of our thinking and remain for ourselves and for others the guardians of our thoughts” (quoted from Brain). This is the reasoning that persuaded Head, Wilson, Goldstein, and others that any comprehensive theory of language must include explanations in terms not only of cerebral anatomy and physiology but also of the psycholinguistic processes that are involved.
Loss or impairment of the production or comprehension of spoken or written language because of an acquired lesion of the brain. This is the condition called aphasia or dysphasia.
Disturbances of speech and language with diseases that globally affect higher-order mental function, i.e., confusion, delirium, mental retardation, and dementia. Speech and language functions are seldom lost in these conditions but are deranged as part of a general impairment of perceptual and intellectual functions (Chap. 21). Common to this category are certain special disorders of speech, such as mutism as outlined by Geschwind in his article on the “non-aphasic disorders of speech” (1964) and extreme perseveration (palilalia and echolalia), in which the patient repeats, parrot-like, sounds, words, and phrases (see further on). The odd constructs of language and other disorders of verbal communication of schizophrenics and some autistic individuals, extending to the production of meaningless phrases, neologisms, or jargon, are probably best included in this category as well but they derive from a disorder of thought.
A defect in articulation with intact mental functions, and comprehension of spoken and written language and normal syntax (grammatical construction of sentences). This is a pure motor disorder of the muscles of articulation and may be a result of flaccid or spastic paralysis, rigidity, repetitive spasms (stuttering), or ataxia. The terms dysarthria and anarthria are applied to this category of speech disorder.
An alteration or loss of voice because of a disorder of the larynx or its innervation—aphonia or dysphonia. Articulation and language are unaffected.
Anatomy of the Language Functions
The conventional teaching, based on correlations between various disorders of language and damage to particular areas of the brain, postulates four main language areas, situated in most persons in the left cerebral hemisphere (Fig. 23-1). The entire language zone that encompasses these areas is perisylvian, i.e., it borders the sylvian fissure. Two language areas are receptive and two are executive, i.e., the latter are concerned with the production (output) of language. The main receptive area, subserving the perception of spoken and probably of internal language, occupies the posterosuperior temporal area (the posterior portion of area 22) and Heschl gyri (areas 41 and 42). The posterior part of area 22 in the planum temporale is referred to as Wernicke area. A second receptive area occupies the angular gyrus (area 39) in the inferior parietal lobule, anterior to the visual receptive areas. The supramarginal gyrus, which lies between these auditory and visual language “centers,” and the inferior temporal region, just anterior to the visual association cortex, are probably part of the language apparatus as well. Here are located the integrative centers for cross-modal visual and auditory language functions.
Figure 23-1.
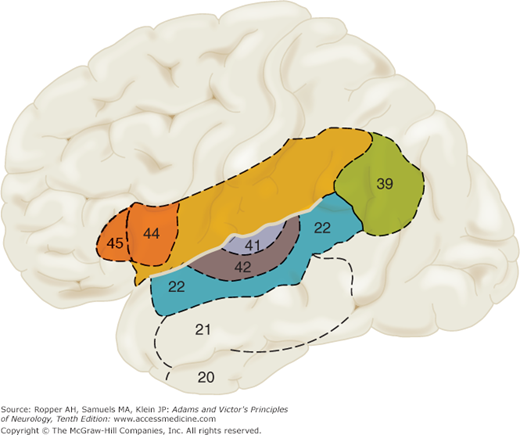
Diagram of the brain showing the classic language areas, numbered according to the scheme of Brodmann. The elaboration of speech and language probably depends on a much larger area of cerebrum, indicated roughly by all the shaded zones (see text). Note that areas 41 and 42, the primary auditory receptive areas, are shown on the lateral surface of the temporal lobe but extend to its superior surface, deep within the sylvian fissure.
The main executive, or output, region, situated at the posterior end of the inferior frontal convolution (Brodmann areas 44 and 45), is referred to as Broca area and is concerned with motor aspects of speech. In some models of language, visually perceived words are given expression in writing through a fourth language area, the so-called Exner writing area in the posterior part of the second frontal convolution. However, this latter concept is controversial in view of the fact that widely separated parts of the language zone may cause a disproportionate disorder of writing. In any case, there are two parallel systems for understanding the spoken word and producing speech and for the understanding of the written word and producing writing. They develop separately but are the integral components of the semantic system.
These sensory and motor language areas are intricately connected with one another by a rich network of nerve fibers, one large bundle of which, the arcuate fasciculus, passes through the isthmus of the temporal lobe and around the posterior end of the sylvian fissure; other connections may traverse the external capsule of the lenticular nucleus (subcortical white matter of the insula). Many additional corticocortical connections lead into the perisylvian zones and project from them to other parts of the brain. Of special importance for the production of speech are the short association fibers that join the Broca area with the lower rolandic cortex, which, in turn, innervates the muscles of the lips, tongue, pharynx, and larynx. The perisylvian language areas are also connected with the striatum and thalamus and with corresponding areas in the nondominant cerebral hemisphere through the corpus callosum and anterior commissure (see Fig. 22-6).
Having indicated the main regions involved with language, there remains considerable difference of opinion concerning the status of cortical language areas, and objection has been made to calling them “centers,” for they do not represent histologically or circumscribed structures of constant function. Moreover, a neuroanatomist would not be able to distinguish the cortical language areas microscopically from the cerebral cortex that surrounds them.
Knowledge of the anatomy of language has come almost exclusively from the postmortem study of humans with focal brain diseases. Two major theories have emerged from these studies. One has subdivided the language zone into separate afferent (auditory and visual) receptive parts, connected by identifiable tracts to the executive (efferent–expressive) centers. Depending on the exact location of the lesions, a number of special syndromes are elicited. The other broad theory, advanced originally by Marie (he later claims to have changed his mind) and supported by Head, Wilson, Brain, and Goldstein, favored the idea of a single language mechanism, roughly localized in the opercular, or perisylvian region of the dominant cerebral hemisphere. The aphasia in any particular case was presumed to be a result of the summation of damage to input or output modalities relative to this central language zone. Undeniably, there is recognizable afferent and efferent localization within the perisylvian language area, as discussed above, but there is also an undifferentiated central integrative mass action, in which the degree of deficit is to a considerable extent influenced by the size of the lesion. In addition, a strict division of aphasias into expressive and receptive, while still a strong practical concept, is not fully borne out by clinical observation. Nevertheless, there are several localizable language functions in the perisylvian cortex.
Carl Wernicke more than any other person must be credited with the anatomic–psychologic scheme upon which many contemporary ideas of aphasia rest. Earlier, Paul Broca (1865), and, even before him, Dax (1836), made the fundamental observations that a lesion of the insula and the overlying operculum deprived a person of speech and such lesions were always in the left hemisphere. Wernicke’s thesis was that there were two major anatomic loci for language: (1) an anterior locus, in the posterior part of the inferior frontal lobe (Broca’s area), in which were contained the “memory images” of speech movements, and (2) the insular region and adjoining parts of the posterior perisylvian cortex, in which were contained the images of sounds. (Meynert had already shown that aphasia could occur with lesions in the temporal lobe, the Broca area being intact.) Wernicke believed that the fibers between these regions ran in the insula and mediated the reflex arc between the heard and spoken word. Later, Wernicke came to accept von Monakow’s view that the connecting fibers ran around the posterior end of the sylvian fissure, in the arcuate fasciculus. Wernicke gave a comprehensive description of the receptive, or sensory, aphasia that now bears his name. The four main features he pointed out were (1) a disturbance of comprehension of spoken language and (2) of written language (alexia), (3) agraphia, and (4) fluent paraphasic speech. In Broca’s aphasia, by contrast, comprehension was intact, but the patient was mute or employed only a few simple words. Wernicke also theorized that a lesion interrupting the connecting fibers between the two cortical speech areas would leave the patient’s comprehension undisturbed but would prevent the intact sound images from exerting an influence on the choice of words. Wernicke proposed that this variety of aphasia be called Leitungsaphasie, or conduction aphasia (called central aphasia by Kurt Goldstein and deep aphasia by Martin and Saffran). Careful case analyses since the time of Broca and Wernicke have borne out these associations between a receptive (Wernicke) type of aphasia and lesions in the posterior perisylvian region and between a predominantly (Broca) motor aphasia and lesions in the posterior part of the inferior frontal lobe and the adjacent, insular, and opercular regions of the frontal cortex. We have certainly encountered cases that conform to the Wernicke model of conduction aphasia; the lesion in these cases may lie in the parietal operculum, involving the white matter deep to the supramarginal gyrus, where it presumably interrupts the arcuate fasciculus and posterior insular subcortex (the issue of conduction aphasia is discussed further on).
How these regions of the brain are organized into separable but interactive modules, resulting in the complex behavior of which we make daily use in interpersonal communication, is still being studied by linguists and cognitive neuropsychologists. They have dissected language into its most basic elements—phonemes (the smallest units of sound recognizable as language), morphemes (the smallest meaningful units of a word), graphemes, lexical and semantic elements (words and their meanings), and syntax (sentence structure). In general, as a restatement of the Wernicke-Broca scheme, phonologic speech output difficulties are derived from left frontal lesions; semantic–comprehension difficulties are the result of left temporal lesions; and alexia and agraphia are associated with inferior parietal lesions. These “modules” of language have been diagrammed by psycholinguists as a series of boxes and are connected to one another by arrows to indicate the flow of information and the manner in which they influence the spoken output of language. “Boxologies,” as they are called, are consistent with current cognitive theory, which views language functions as the result of synchronized activity in vast neuronal networks made up of many cerebrocortical regions and their interconnecting pathways (Damasio and Damasio, 1989).
On the other hand, despite this level of theoretical sophistication, attempts to delineate the anatomy of speech and language disorders by means of conventional brain imaging techniques in aphasic patients have been somewhat disappointing. In early studies using CT, LeCours and Lhermitte were unable to establish a consistent correspondence between the type of aphasia and the location of the demonstrable lesion. Similarly, Willmes and Poeck, in a retrospective study of 221 aphasic patients, failed to find an unequivocal association between the type of aphasia and the CT localization of the lesion. These poor correlations are in part related to the timing and the crudity of the CT scan. MRI scans performed soon after a stroke show somewhat more consistent correlations between the type of language disturbance and the location of lesions in the perisylvian cortex, but lesions in identical locations may produce functionally different language disorders. Functional magnetic resonance imaging (fMRI), while subjects are engaged in language production and comprehension, provides an additional perspective for understanding the language process, but so far only the broadest rules of localization can be confirmed. Studies of blood flow and topographic physiology during the acts of reading and speaking, while generally affirming nineteenth-century models of language, have shown widespread activation of Wernicke and Broca areas, as well as of the supplementary motor area and areas of the opposite hemisphere (see Price).
Although localization of the lesion that produces aphasia is in most instances roughly predictable from the clinical deficit, there are wide variations. The inconsistency has several explanations, one being that the net effect of any lesion depends not only on its locus and extent but also on the degree of cerebral dominance, i.e., on the degree to which the nondominant hemisphere assumes language function after damage to the dominant one. According to this view, a left-sided lesion has less effect on language function if cerebral dominance is poorly established than if dominance is strong. In all likelihood, the variability between patients in lesion location and the characteristics of aphasia has to do with subtle differences in the organization of the language cortices. Another explanation invokes the poorly understood concept that individuals differ in the ways in which they acquire language as children. This is believed to play a role in making available alternative means for accomplishing language tasks when the method initially learned has been impaired through brain disease. The extent to which improvement of aphasia represents “recovery” of function or generation of new modes of response has not been settled.
Cerebral Dominance and Its Relation to Language and Handedness
The functional supremacy of one cerebral hemisphere is fundamental to language function. There are many ways of determining that the left side of the brain is dominant: (1) by the loss of speech that occurs with disease in parts of the left hemisphere and its preservation with lesions involving corresponding parts of the right hemisphere; (2) by preference for and greater facility in the use of the right hand, foot, and eye; (3) by the arrest of speech with a focal seizure or with electrical or magnetic stimulation of the anterior (left) language area; (4) by the injection of sodium amytal or an equivalent drug into the left internal carotid artery (the Wada test—a procedure that produces mutism for a minute or two, followed by misnaming, including perseveration and substitution; misreading; and paraphasic speech); (5) by dichotic listening, in which different words or phonemes are presented simultaneously to the two ears (yielding a right ear–left hemisphere advantage); (6) by observing increases in cerebral blood flow during language processing; and (7) by lateralization of speech and language functions following commissurotomy.
Language hemisphere dominance is ostensibly related to hand dominance, but this is more of a supposition than a statement. Approximately 90 to 95 percent of the general population is right-handed; i.e., they innately choose the right hand for intricate, complex acts and are more skillful with it. The preference is more complete in some persons than in others. Most individuals are neither completely right-handed nor completely left-handed but strongly favor one hand for more complicated tasks. The reason for hand preference is not fully understood. There is strong evidence of a hereditary factor but the mode of inheritance is uncertain. Learning is also a factor; many left-handed children are shifted at an early age to right (shifted sinistrals) because it had been a perceived handicap to be left-handed in a right-handed world. Most right-handed persons, when obliged to use only one eye (looking through a keyhole, gun sight, telescope, etc.), sight with the right eye, and it has been stated that eye preference coincides with hand preference. Even if true, this still does not account for hemispheral dominance. It is, however, noteworthy that handedness develops simultaneously with language. The most that can be said at present is that localization of language and a preference for one eye, hand, and foot, as well as praxis, are all manifestations of some fundamental, partly inherited tendency for hemispheric specialization.
There are slight but definite anatomic differences between the dominant and the nondominant cerebral hemispheres. Yakovlev and Rakic, in a study of infant brains, observed that the corticospinal tract coming from the left cerebral hemisphere contains more fibers and decussates higher than the tract from the right hemisphere. More pertinent to language, the planum temporale, the region on the superior surface of the temporal lobe posterior to Heschl gyri and extending to the posterior end of the sylvian fissure, is slightly larger on the left in 65 percent of brains and larger on the right in only 11 percent (Geschwind and Levitsky). LeMay and Culebras noted in cerebral angiograms that the left sylvian fissure is longer and more horizontal than the right and that there is a greater mass of cerebral tissue in the area of the left temporoparietal junction. CT scanning has shown the right occipital horn to be smaller than the left, indicative perhaps of a greater right-sided development of visuospatial connections. Also, subtle cytoarchitectonic asymmetries of the auditory cortex and posterior thalamus have been described; these and other biologic aspects of cerebral dominance have been reviewed by Geschwind and Galaburda particularly as they relate to developmental dyslexia (Chap. 28).
Left-handedness may result from disease of the left cerebral hemisphere in early life; this probably accounts for its higher incidence among the mentally retarded and brain injured. Presumably, the neural mechanisms for language then come to be represented during early development in the right cerebral hemisphere. Handedness and cerebral dominance may fail to develop in some individuals; this is particularly true in certain families. In these individuals, defects in reading as well as the faults of stuttering, mirror writing, and general clumsiness are frequent. In right-handed individuals, aphasia is almost invariably related to a left cerebral lesion; aphasia in such individuals as a result of purely right cerebral lesions (“crossed aphasia”) is very rare, occurring in only 1 percent of cases (Joanette et al). Cerebral language dominance in ambidextrous and left-handed persons is not nearly so uniform. In a large series of left-handed patients with acquired aphasia, 60 percent had lesions confined to the left cerebral hemisphere (Goodglass and Quadfasel). Furthermore, in the relatively rare case of aphasia caused by a right cerebral lesion, the patient is nearly always left-handed and the language disorder is less severe and less enduring than in right-handed patients with comparable lesions in the left hemisphere (Gloning; Subirana). Taken together, these findings suggest a bilateral—albeit unequal—representation of language functions in non–right-handed patients. This has been affirmed by the Wada test; Milner and colleagues found evidence of bilateral speech representation in 32 (about 15 percent) of 212 consecutive left-handed patients.
The undoubted language capacities of the nondominant hemisphere have been documented by lesional neurology. In cases of congenital absence (or surgical section) of the corpus callosum, which permits the testing of each hemisphere, there has been virtually no demonstrable language function of the right hemisphere. However, Levine and Mohr found that the nondominant hemisphere retains a limited capacity to produce oral speech after extensive damage to the dominant hemisphere; their patient recovered the ability to sing, recite, curse, and utter one- or two-word phrases, all of which were completely abolished by a subsequent right hemisphere infarction. The fact that varying amounts of language function may remain after dominant hemispherectomy in adults with glioma also suggests a definite though limited capacity of the adult nondominant hemisphere for language production. Kinsbourne’s observations of the effect of sodium amytal injections into the right-hemispheral arteries of patients who are aphasic from left-sided lesions make the same point.
Despite its minimal contribution to the purely linguistic or propositional aspects of language, the right hemisphere does have a role in the implicit communication of emotion through the subtleties of propositional language. These modulative aspects of language are subsumed under the term prosody, by which is meant the melody of speech, its intonation, inflection, and pauses, all of which have emotional overtones. The prosodic components of speech and the gestures that accompany them enhance the meaning of the spoken word and endow speech with its richness and vitality. The related issue of an individual’s accent, which carries such a strong regional identity and is acquired early in life, may also have an anatomic basis, but one that remains obscure (see later comments on the “Foreign Accent Syndrome”).
Many diseases and focal cerebral lesions mute or reduce the prosody of speech, the most dramatic examples being the hypophonic monotone of Parkinson disease and the effortful utterances of Broca’s aphasia. Largely through the work of Ross, it has become apparent that prosody is also greatly disordered in patients with strokes involving portions of the nondominant hemisphere that mirror the language areas of the left hemisphere. In these cases, there is impairment both of comprehension and of production of the emotional content of speech and its accompanying gestures. A prospective study of middle cerebral artery infarctions by Darby corroborated this view: aprosodia, as it has come to be called, was present only in those patients with lesions in the territory of the inferior division of the right middle cerebral artery. The deficit was most prominent soon after the stroke and was not found with lacunar lesions. In our patients, using bedside tests, we have had difficulty in appreciating aprosodia as a result solely of right perisylvian lesions, and in most cases, the damage has been more widespread.
There has been recent interest in a role for the cerebellum in language function, based partly on observations in the Williams syndrome, in which mental retardation is associated with a preservation of language skills that is sometimes striking in degree (Chap. 38). In this disease, the cerebellum is spared in the face of greatly diminished volume of the cerebral hemispheres (see Leiner et al). Some studies of cerebral blood flow also implicate the cerebellum in various language functions; based on our clinical experience, however, we would judge any language deficits from cerebellar disease to be subtle or nonexistent. Dysarthria, of course, is common with cerebellar disease.
Approach to the Patient with Language Disorders
In the investigation of aphasia, it is first necessary to inquire into the patient’s native language, handedness, and previous level of literacy and education. It has been surmised that following the onset of aphasia, individuals who had been fluent in more than one language (polyglots) improved more quickly in their native language than in a subsequently acquired one (a derivative of the Ribot law of retained distant memory). This rule seems to hold if the patient is not truly fluent in the more recently acquired language or has not used it for a long time. More often, the language most used before the onset of the aphasia will recover first (Pitres law). Usually, if adequate testing is possible, more or less the same aphasic abnormalities are found in both the first and the more recently acquired language. Dementing illnesses such as Alzheimer disease, however, do cause increasing use of the first acquired language.
Many naturally left-handed children are trained to use the right hand for writing; therefore, in determining handedness, one must ask which hand is preferred for throwing a ball, threading a needle, sewing, or using a tennis racket or hammer, and which eye is used for sighting a target with a rifle or other instrument. It is important, before beginning the examination, to determine whether the patient is alert and can participate reliably in testing, as accurate assessment of language depends on these factors.
One should quickly ascertain whether the patient has other gross signs of a cerebral lesion such as hemiplegia, facial weakness, homonymous hemianopia, or cortical sensory loss. When a constellation of these major neurologic signs is present, the aphasic disorder is usually of the total (global) type. A right brachiofacial paralysis aligns with Broca’s aphasia; in contrast, a restricted right hemianopia or quadrantanopia is a common accompaniment of Wernicke’s aphasia, and hemiparesis is absent. Dyspraxia of limbs and speech musculature in response to spoken commands or to visual mimicry is generally associated with Broca’s aphasia, but sometimes with Wernicke’s aphasia. Homonymous hemianopia without motor weakness tends often to be linked to pure word blindness, to alexia with or without agraphia, and to anomic aphasia.
The bedside analysis of aphasic disorders that we find most useful entails the systematic testing of six aspects of language function: conversational speech, comprehension, repetition, reading, writing, and naming. Simply engaging the patient in conversation permits assessment of the motor aspects of speech (praxis and prosody), fluency, and language formulation. If the disability consists mainly of sparse, laborious, nonfluent speech, it suggests, of course, Broca’s aphasia, and this possibility can be pursued further by tests of repeating from dictation and by special tests of praxis of the oropharyngeal muscles. Fluent but empty paraphasic speech with impaired comprehension is indicative of Wernicke’s aphasia. Impaired comprehension but perfectly normal formulated speech and intact ability to read suggest the rare syndrome of pure word deafness.
When conversation discloses virtually no abnormalities, other tests may still be revealing. The most important of these are reading, writing, repetition, and naming. Reading aloud single letters, words, and text may disclose the dissociative syndrome of pure word blindness. Except for this syndrome and isolated mutism (aphemia; see earlier), writing is disturbed in all forms of aphasia. Literal and verbal paraphasic errors may appear in milder cases of Wernicke’s aphasia as the patient reads aloud from a text or from words in the examiner’s handwriting. Similar errors appear even more frequently when the patient is asked to explain the text, read aloud, or give an explanation in writing.
Testing the patient’s ability to repeat spoken language is a simple and important maneuver in the evaluation of aphasic disorders. As with other tests of aphasia, it may be necessary to increase the complexity of the test from digits and simple words to complex words, phrases, and sentences to disclose the full disability. Defective repetition occurs in all the major forms of aphasia (Broca’s, Wernicke’s, and global) because of lesions in the perisylvian language areas. The patient may be unable to repeat what is said to him, despite relatively adequate comprehension—the hallmark of conduction aphasia. Contrariwise, normal repetition in an aphasic patient (transcortical aphasia) indicates that the perisylvian area is largely intact. In fact, the tendency to repeat may be excessive (echolalia). Preserved repetition is also characteristic of anomic aphasia and occurs occasionally with subcortical lesions. Disorders confined to naming, other language functions (reading, writing, spelling) being adequate, are diagnostic of amnesic, or anomic, aphasia and referable usually to lower temporal lobe lesions.
These deficits can be quantified by the use of any one of several examination procedures. Those of Goodglass and Kaplan (Boston Diagnostic Aphasia Examination [BDAE]) and of Kertesz (Western Aphasia Battery [WAB]) are the most widely used in the United States. The use of these procedures will enable one to predict the type and localization of the lesion in approximately two-thirds of the patients, which is not much better than detailed bedside examination. Using these tests, aphasia of the Broca, Wernicke, conduction, global, and anomic types accounted for 392 of 444 unselected cases studied by Benson.
Clinical Varieties of Aphasia
In analyzing disorders of speech and language in the clinic or at the bedside, the first objective is to separate dysarthria, or slurred speech with preservation of language, from a genuine impairment in language function, aphasia. Here, we offer a practical approach to aphasia. Dysarthria is addressed in a later section. To recapitulate, the features of a language disorder that are used to advantage by the examiner in determining the type of aphasia are:
- natural sounding fluency, including normal cadence, the use of prepositions, and correct grammar;
- comprehension of language;
- the proper selection, use, and relationships between words;
- naming of displayed objects;
- the ability to repeat in comparison to spontaneous speech;
- reading; and
- writing
This type of systematic examination will enable one to decide whether a patient has a predominantly: (i) motor or Broca’s aphasia, sometimes called “expressive,” “anterior,” or “nonfluent” aphasia; (ii) sensory or Wernicke’s aphasia, referred to also as “receptive,” “posterior,” or “fluent” aphasia; (iii) a total or global aphasia, with loss of all or nearly all speech and language functions; (iv) transcortical aphasia, meaning a motor or sensory aphasia with preserved repetition; or (v) one of the disconnection language syndromes, such as conduction aphasia, word deafness (auditory verbal agnosia), and word blindness (visual verbal agnosia or alexia). In addition, there is a condition of mutism, or a complete absence of verbal output, but this syndrome does not permit one to predict the exact locus of the lesion. Anomia (also called nominal or amnesic aphasia, meaning loss of naming ability) and the impaired ability to communicate by writing (agraphia) are found to some degree in practically all types of aphasia. As for agraphia, it rarely exists alone. Table 23-1 summarizes these main aphasic syndromes, which are described below. Even though these descriptions are based largely on deficits from vascular occlusion, they serve well in most circumstances of focal brain disease that cause language disturbances.
TYPE OF APHASIA | SPEECH | COMPREHENSION | REPETITION | ASSOCIATED SIGNS | LOCALIZATIONa |
|---|---|---|---|---|---|
Broca’s | Nonfluent, effortful, agrammatical, paucity of output but transmits ideas | Relatively preserved | Impaired | Right arm and face weakness | Frontal suprasylvian |
Wernicke’s | Fluent, voluble, well articulated but lacking meaning | Greatly impaired | None | Hemi- or quadrantanopia, no paresis | Temporal, infrasylvian including angular and supramarginal gyri |
Conduction | Fluent | Relatively preserved | None | Usually none | Supramarginal gyrus or insula |
Global | Scant, nonfluent | Very impaired | None | Hemiplegia usual | Large perisylvian or separate frontal and temporal |
Transcortical motor | Nonfluent | Good | Largely preserved |







