2 Cognitive and Language Evaluation
Introduction
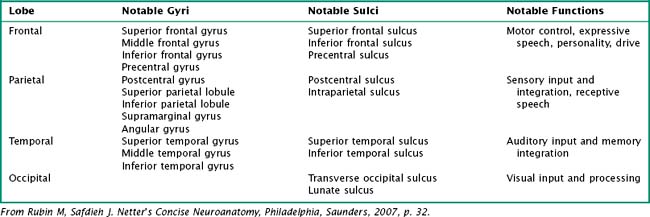
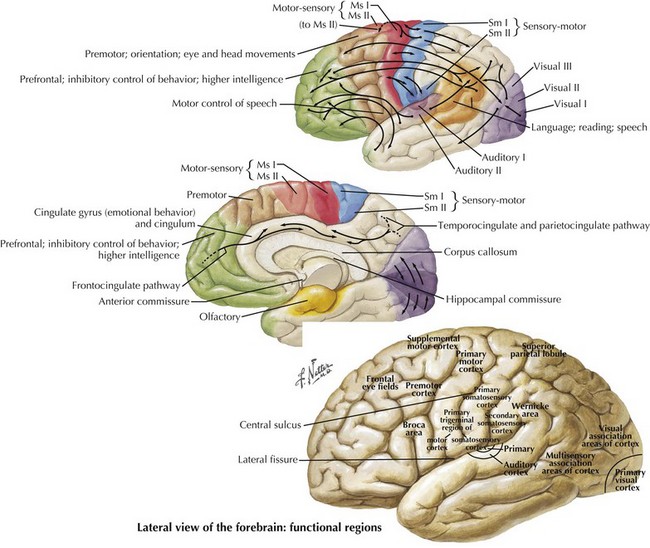
One’s direct interaction with the patient helps define the behavioral aspects of neurologic function; it is their mood, affect, level of cooperation, and distractibility that are noteworthy. The cognitive part of the neurologic evaluation strives to determine the precise level of various higher cortical functions. The human cerebral cortex, with its multiple gyri and network of many million interconnections, is the most complex part of the brain. Anatomically, the cortex is classified into four major functional areas: frontal, temporal, parietal, and occipital lobes (Fig. 2-1; Table 2-1 and Table 2-2). These anatomic substrates are carefully interconnected in a complex network. Although for the sake of discussion, these cortical areas are typically described in isolation, in reality these interconnections with other cortical and subcortical areas are critical for brain function (Fig. 2-2).
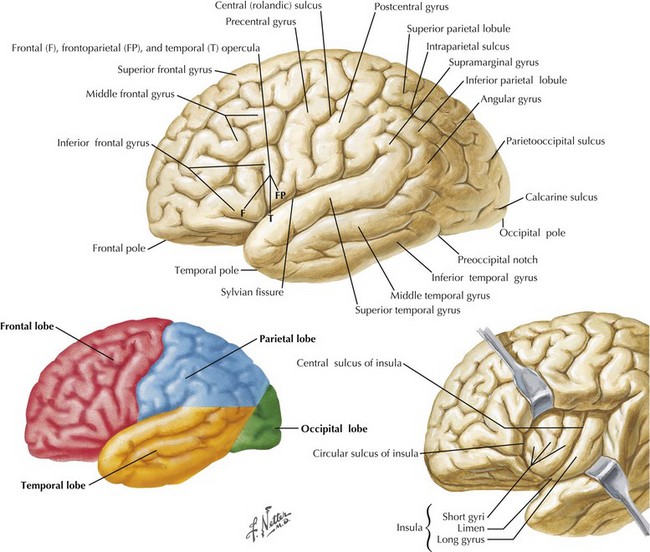
Table 2-1 Lateral Surface of the Brain: Notable Lateral Sulci
| Structure | Anatomic Significance |
|---|---|
| Lateral (Sylvian) fissure | Separates temporal lobe from frontal and parietal lobes |
| Central (Rolandic) sulcus | Separates frontal lobe from parietal lobe |
From Rubin M, Safdieh J. Netter’s Concise Neuroanatomy, Philadelphia, Saunders, 2007, p. 32.
Cognitive Testing
An Introductory Mental Status Examination
There are several standardized brief assessments of cognition, including the Mini Mental State Exam and the Montreal Cognitive Assessment (MOCA). These studies are particularly useful for assessing memory problems in the elderly. The MOCA is available online at www.mocatest.org along with normative data and translation into multiple languages. It is very useful when screening for very subtle cognitive impairment as seen in Mild Cognitive Impairment or the very earliest stages of dementia. The MMSE may provide a useful tool for staging dementia severity in patients with Alzheimer disease. Additional discussion of such tests is presented in the subsequent dementia chapter (Chapter 18).
Frontal Lobe Dysfunction
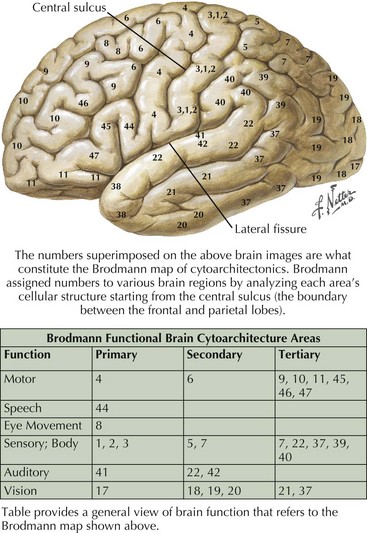
The frontal lobe comprises the major portion of the adult brain occupying approximately 30% of brain mass. This includes the motor area (Brodmann area 4), the premotor cortex (Brodmann areas 6 and 8), and significant prefrontal areas (Fig. 2-3). A Brodmann area is a region of the cortex that is defined by the organization of its cells, or cytoarchitecture, as opposed to gross anatomic landmarks such as sulci or gyri. Reference to Brodmann’s areas may provide more precise clinicoanatomic correlation and localization (see Fig. 2-3).
The significant prefrontal areas are distinct from the adjacent motor and premotor areas, particularly in their connections with other cortical areas and the thalamus (see Fig. 2-2). Most of the prefrontal–thalamic connections are made with the dorsal medial nucleus, a prime relay center for limbic projections originating from the amygdala and the basal forebrain. The reciprocal inputs are the most prominent cortical connections, originating from second-order sensory association and paralimbic association areas, including the cingulate cortex, temporal pole, and parahippocampal area. The frontal lobe is an integrator and analyzer of highly complex multimodal cortical areas, including limbically processed information.
Humans sustaining frontal lobe disorders develop significant personality changes and “release of animal instincts.” One of the earliest descriptions of frontal lobe damage described patients with apathy and disturbed emotions. Elucidation of the frontal lobe connections, particularly the medial-basal portion, demonstrates that the limbic system provides significant input to that area (Fig. 2-4). Autonomic centers originating in the brainstem and hypothalamus also have significant connections with the basal frontal lobe. When these connections are disrupted, aggressive, impulsive, and uncontrolled behavior results. Subsequent study has revealed an even greater depth and breadth of frontal lobe function.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


