♦ Preoperative
Determine Appropriateness of Costotransversectomy
- Advantages of costotransversectomy
- Less extensive than thoracotomy
- Adequate for pathology along lateral canal up to midline
- Less extensive than thoracotomy
- Disadvantages of costotransversectomy
- Cannot access pathology across midline of canal
- Significant paraspinal muscle dissection
- Cannot access pathology across midline of canal
Imaging
- Plain x-rays
- Determine number of ribs for localization
- Assess deformity and/or instability
- Determine number of ribs for localization
- Magnetic resonance imaging (MRI)
- Determine extent of neural element compression
- Computed tomography
- Evaluate bony anatomy
- Computed tomography/myelogram
- If MRI is contraindicated
Operative Planning
- Patient counseling regarding risk, benefits, and postoperative course
Routine Equipment
- Basic spine tray including Kerrison rongeurs (2 to 4 mm)
- Cautery–monopolar and bipolar
- High-speed drill (e.g., Midas Rex)
- Headlight and loupe magnification
- Table-mounted retractor (Thompson-Farley [Thompson Surgical Instruments, Inc., Traverse City, MI] versus Omni-Tract [Omni-Tract Surgical, St. Paul, MN])
- Cell Saver–if significant blood loss is anticipated in the absence of infection/neoplastic disease
- Microscope for intradural pathology
- Spinal instrumentation if reconstruction is intended
Operating Room Set-up
- Prone table: Jackson table with Wilson frame or bolsters
- Make sure patient is secured well in case rotation of the table is required
- Mayfield head holder versus Gardner-Wells tongs with traction
- Intraoperative anteroposterior and lateral x-ray versus fluoroscopy
Anesthetic Issues
- Secure endotracheal tube for prone position
- Appropriate blood pressure monitoring
- Foley catheter for extended cases (beyond 3 hours)
- Perioperative antibiotics 30 minutes prior to skin incision
- Perioperative steroids for decompressive or intradural pathology
- Avoid any orbital compression if patient’s face is placed on cushioned mask
♦ Intraoperative
Positioning
- Options
- Standard prone position
- Three quarter prone with side of pathology elevated
- Standard prone position
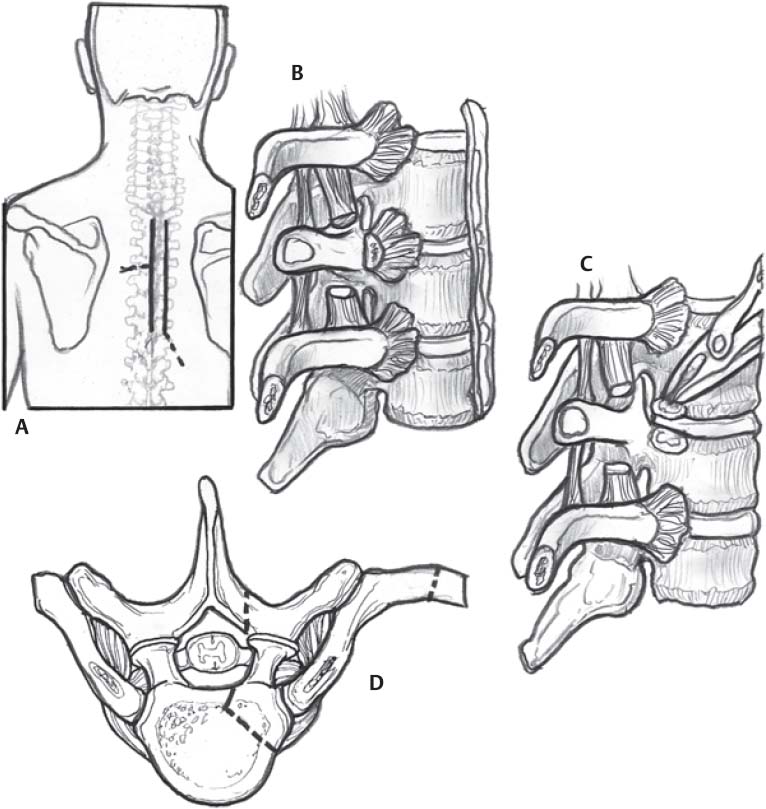
Incision
- Options
- Curvilinear incision, beginning and ending in the midline with apex centered over the rib to be resected, ~5 to 7 cm from midline
- Midline incision: requires extended length to mobilize paraspinal muscles
- Paramedian incision several centimeters from the midline
- Curvilinear incision, beginning and ending in the midline with apex centered over the rib to be resected, ~5 to 7 cm from midline
Planning of Sterile Preparation
- Standard scrub and prep
Exposure
- Incision taken through subcutaneous tissue and transect muscles including trapezius/latissimus dorsi/rhomboids in line with skin incision
- Dissection continued to identify rib of interest
- Erector spinae muscles are mobilized through medial and lateral dissection off of the posterior spinal elements including the spinous process, lamina, and transverse process to allow medial retraction of the muscle.
- Confirm localization with intraoperative imaging.
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


