3 Cranial Nerve I
Olfactory
Dysfunction of the olfactory nerve is quite rare, occurring in certain very select circumstances. Examination of olfactory function is not routinely pursued during the average neurologic evaluation (Chapter 1). However, in clinical settings such as in the above vignette, it is essential to routinely evaluate olfactory function by asking the patient to identify a few familiar odors such as coffee, perfumes, tobacco, etc. On occasion, the patient may not be aware of or assign much importance to the loss of his or her smell sensation. This may be particularly true when there is a concomitant neurologic deficit as seen in occasional patients with potentially treatable olfactory groove meningiomas that also compromise frontal lobe function.
Anatomy
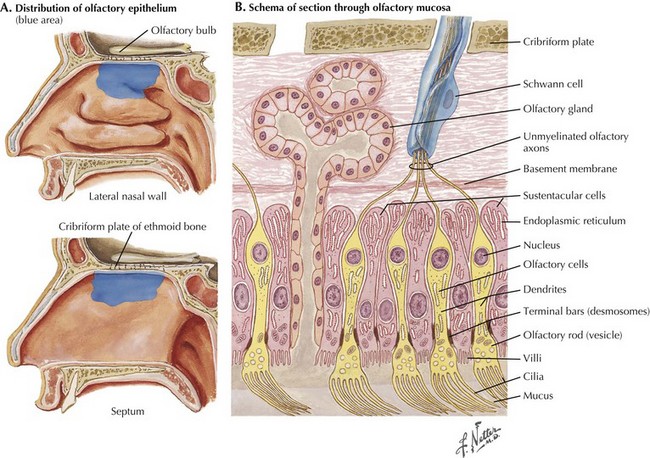
When identifying odors, humans rely on volatile substances entering their nasal cavity to excite receptors. Olfactory receptor cells are bipolar sensory neurons whose dendrites form a delicate sensory carpet on the superior aspect of the nasal cavity (Fig. 3-1). The thin, unmyelinated axons of the bipolar sensory cells collectively form the olfactory nerve. These travel through the cribriform plate into the olfactory bulb at the base of the fronto-orbital lobe. Within the bulb, CN-I fibers synapse with the dendrites of the large mitral cells, whose axons constitute the olfactory tract passing along the base of the frontal lobe and projecting directly into the primary olfactory cortex within the temporal lobe. In contrast to all other sensory modalities, olfactory sensation does not have a central processing site such as within the thalamic nuclei (Fig. 3-2). This direct pathway to the cerebral limbic structures may have had an important evolutionary function in lower animals and, later, primates.
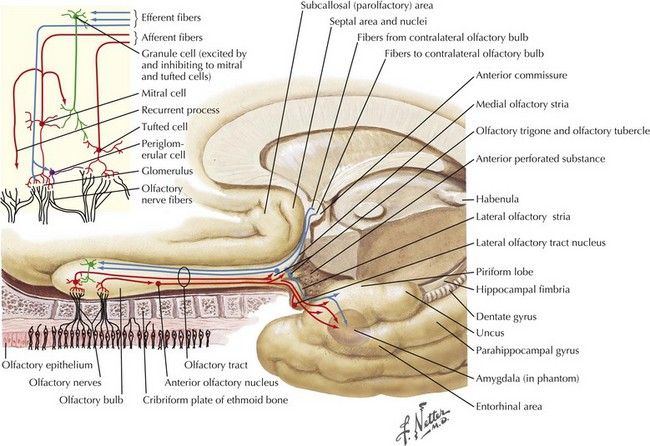
The human primary olfactory cortex includes the uncus, hippocampal gyrus, amygdaloid complex, and entorhinal cortex (Fig. 3-2). Cortical representation of smell is bilateral. Although most of the olfactory tract fibers supply the ipsilateral olfactory cortex, some fibers decussate in the anterior commissure and terminate in the opposite hemisphere. Consequently, a unilateral lesion distal to the decussation rarely produces any olfactory dysfunction.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


