10 Cranial Nerves XI and XII
Accessory and Hypoglossal
Cranial Nerve XI: The Spinal Accessory Nerve
Anatomy
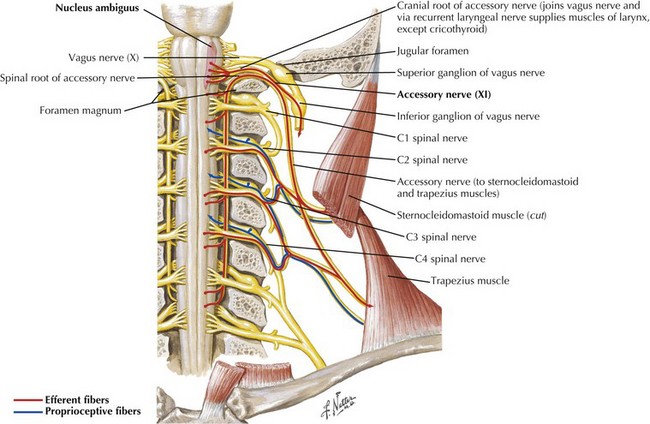
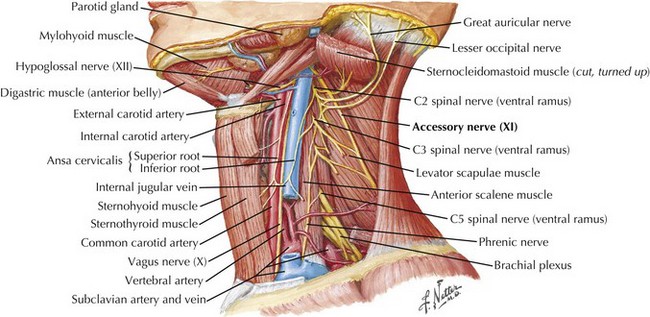
The SAN is primarily a motor nerve innervating the SCM and trapezius muscles in the neck and back (Fig. 10-1). In contrast to the other cranial nerves, its lower motor neuron cell bodies are located primarily within the spinal cord. The accessory nucleus is a cell column within the lateral anterior gray column of the upper five or six cervical spinal cord segments. Proximally it lies nearly in line with the nucleus ambiguus and caudally within the dorsolateral ventral horn. Originating from the accessory nucleus, the rootlets emerge from the cord and unite to form the trunk of CN-XI. This extends rostrally through the foramen magnum into the posterior cranial fossa. Intracranially, it accompanies the caudal fibers of the vagus nerve (CN-X) exiting the skull through the jugular foramen. The SAN then descends in close proximity to the internal carotid artery and internal jugular vein (Fig. 10-2).
The supranuclear innervation of the CN-XI nuclei is still a matter of debate. Although the trapezius muscle is innervated from the opposite hemisphere, there is some question as to whether the supranuclear innervation of the SCM is also contralateral. One standard neuroanatomy text, Brodal 1998, states that with clinical corticobulbar lesions there is paresis of the contralateral SCM as well as the trapezius. Others note, based on intracarotid Amytal injections, that the SCM is innervated predominantly from the ipsilateral hemisphere. Suffice it to say that the most proximal and midline musculature can be activated bilaterally. Therefore, one needs to be circumspect when attempting to lateralize the source of unilateral SCM weakness.
Clinical Presentation and Diagnostic Approach
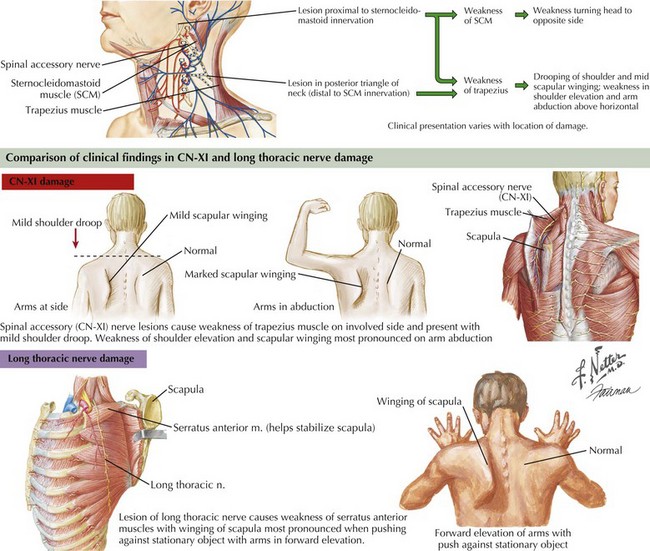
Involvement of the trapezius manifests as drooping of the shoulder and mild scapular winging away from the chest wall with slight lateral displacement. Weakness in shoulder elevation and arm abduction above horizontal is typical. Winging is apparent with arms hanging along the trunk, and becomes accentuated when patients abduct the arms. In contrast, scapular winging from serratus anterior weakness due to long thoracic nerve palsy is most prominent on forward elevation of the arms (Fig. 10-3).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


