Craniopagus Twins
Craniopagus is among the rarest and most complex congenital abnormalities, with a history detailed in both mythology and contemporary medical literature. The technical ability to separate craniopagus twins did not develop until 1952, and even then only one twin survived the operation. Overall outcomes have been mixed until recently, with one twin of the pair usually experiencing severe neurologic consequences and often death after separation. Although modern neurosurgical techniques have evolved, the separation of craniopagus twins continues to be one of the most challenging and risky procedures in neurosurgery. With the historical record full of surgical misadventures, the decision to separate craniopagus twins poses not only a complex surgical dilemma but rightfully an ethical and philosophical challenge, as well. As additional cases have come to medical attention, two opposing strategies for separation have emerged. As the name implies, single-stage separation involves a single marathon surgery during which physical separation is performed, although preparatory surgeries to expand the scalp may precede the separation. In the last two decades, a new strategy involving multiple-stage separation has developed. In staged separations, multiple craniotomies spread over a period of several months gradually eliminate the venous and tissue connections to permit each child to develop independent cerebral venous drainage. Both single-stage and multiple-stage separation attempts have been vocally advocated as superior, but recent cases have demonstrated improved survival and outcomes with a multiple-stage approach. In this chapter, we provide a historical and epidemiologic perspective on this condition, illustrate strategies for presurgical evaluation, discuss the techniques for separation, with an emphasis on the rationale for the multiple-stage approach, and share examples of cases deemed nonseparable with current techniques and technology. We also briefly discuss the socioeconomic impact of taking on one of these challenging cases and the ethical dilemma raised by the huge allocation of resources needed to undertake a successful separation attempt.
21.1 Craniopagus: Brief Historical Perspective
Notable recent cases and attempted separations have become worldwide spectacles, leveraging our innate curiosity about these individuals and showcasing the most difficult of neurosurgical procedures; however, the same curiosity is manifested in literature and art dating to antiquity. As in the present day, those who survived infancy became the subject of fascination for some and were feared, ridiculed, or exploited by others. The earliest documented case of craniopagus twins dates from the 15th century (▶ Fig. 21.1). These twins were born in Bavaria, Germany, in 1491 and were described as a monestare (“warning from God”).1 In a famous case of craniopagus parasiticus in the 1770s, the twins were known as the boys of Bengal2 (▶ Fig. 21.2). In the early 17th century, it became quite popular to place conjoined twins on exhibit in traveling road shows and circuses as “freaks” of nature. The showmen would also produce and distribute show cards and autographed pictures, thereby generating an extra and significant source of income (▶ Fig. 21.3). Even in the early medical literature, conjoined twins were described as “double monstrosities.”3
Fig. 21.1 Early image of conjoined twins.
(From Cosmographia, by Sebastian Münster (1488–1552), a Basel edition printed by Sebastian Heinrich-Petric in 1550 (see leaves dcclxvii–dccixvii, i.e. 767–768). From the personal collection of J.T.G.)
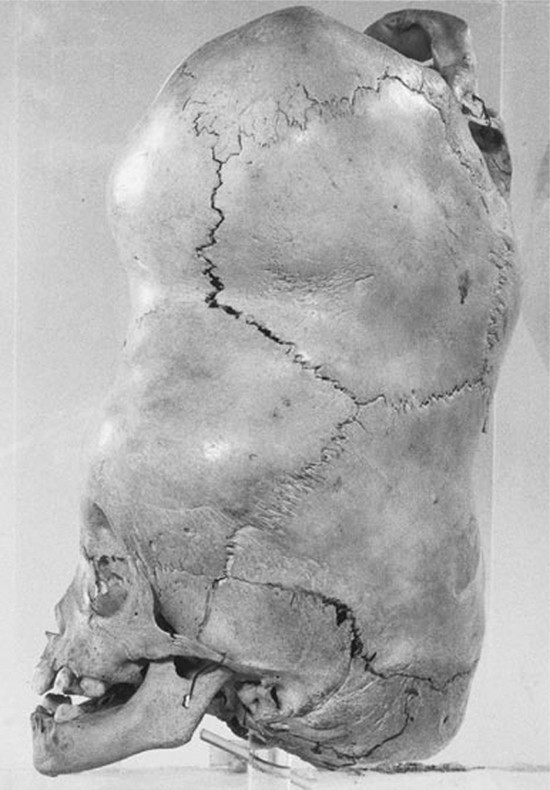
Fig. 21.2 Preserved skull of the boys of Bengal.
(From the Hunterian Collection.)
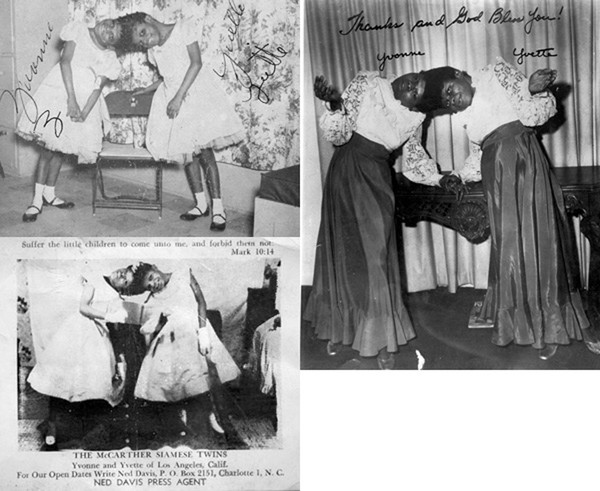
Fig. 21.3 The McCarther twins. Photos such as these were given out at events and affairs. The image at the lower left includes information about the press agent.
(Images from the personal collection of J.T.G.)
Several sets of craniopagus twins have lived into adulthood, although 75% die in the perinatal period and more than 90% have died by the age of 10 years, regardless of attempts at surgical separation.4 The first successful craniopagus surgery in which one twin lived was in 1952–1953. Oscar Sugar, MD, and his team in Chicago undertook the separation of Roger and Rodney Brodie.5,6 Although Roger died 1 month after surgery, Rodney lived to the age of 11 and died of complications of hydrocephalus. The first reported case in which both twins survived was reported just a few years later, in 1957.7 Christine Quigley highlights the history of several cases of craniopagus twins in her book entitled Conjoined Twins.8
21.2 Classification and Demographics of Craniopagus
In 1865, Forster9 introduced the term craniopagus to define twins joined by a union of the calvaria only10 (▶ Fig. 21.4). The union of the cranial vault is rarely symmetric and may involve any location on the head, leading to an infinite variation of configurations This complexity is further complicated by variations in the degree of conjoining or sharing of underlying structures like the meninges, venous sinuses, and cortex, making each case surgically unique (i.e., no two cases are ever equivalent).
Despite of the variation, several authors have attempted to classify the phenotypic archetypes seen in craniopagus. O’Connell was among the first to attempt a classification schema, describing partial craniopagus, in which a limited surface area is affected, with intact or minimal cranial defects, and total craniopagus, in which an extensive surface area is shared, with widely connected cranial cavities. O’Connell further subclassified “vertical” craniopagus (“parietal craniopagus” according to the classification of Bucholz et al.11) into types 1 through 3 based on the degree of cranial rotation. More recently, Stone and Goodrich augmented the partial and total divisions described by O’Connell, defining two additional main subtypes, angular and vertical, to describe the longitudinal angle of connection, regardless of axial rotation, and the facial rotation.4 They suggested that this classification might be used to better predict surgical outcomes based on the complexity of the various vascular interconnections.
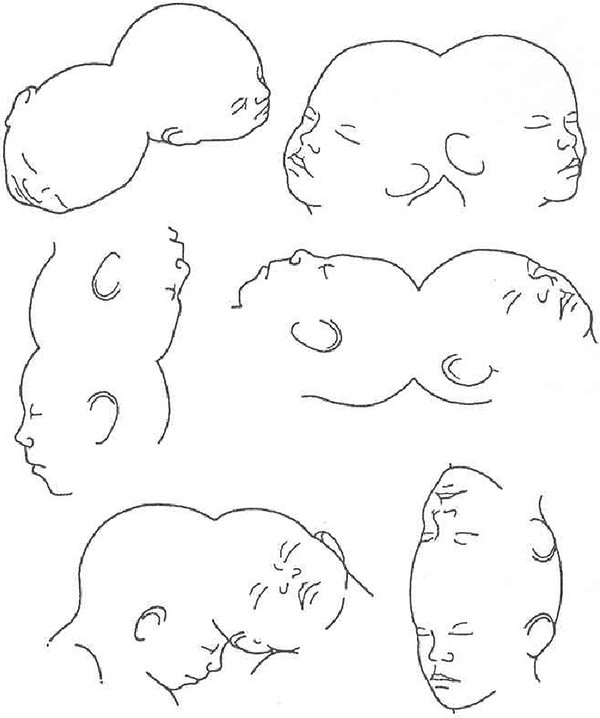
Fig. 21.4 Drawing showing variations on the union in craniopagus twins. (Reproduced from Spencer R. Conjoined Twins: Developmental Malformations and Clinical Implications. Baltimore, MD: Johns Hopkins University Press; 2003.10)
Craniopagus is extremely rare, occurring once in every 0.6 to 2.5 million live births.4,12 The causal factor(s) that lead to craniopagus remain(s) unclear, with various embryologic theories proposed for both “incomplete fission” and “fusion” types.10,13 Although incomplete fission of a fertilized ovum was initially presumed to be the cause of conjoined twins, more current understanding of embryology suggests that the fusion of identical twin embryos during early development is likely the cause. There are no known environmental or genetic factors. The female-to-male ratio is nearly 4:1, but for this, too, no correlative or causal factors are known.
We have previously reported an extensive review of the literature from 1919 through 2006, which noted 64 well-documented cases of craniopagus, with 41 separation attempts. Of these, 29 were performed as a single-stage separation, and 12 separations were attempted with a multiple-stage approach.14
21.3 Risk Stratification of Separation
There are many reports of intra- and extraoperative misadventures; the decision to separate craniopagus twins is one that should be undertaken with serious deliberation and forethought. Until relatively recently, the decision to separate craniopagus twins inherently led to the sacrifice of one of the twins so that the other could live more “normally.” Contemporary management has evolved to the point that a separation attempt is typically offered only if there is a hope of a reasonable outcome for both twins or if the life of one or both of the twins is in danger. As technology and our understanding of the complex craniopagus anatomy has grown, it is now recognized that the presence of shared dural venous sinuses is among the most challenging issues faced in any separation attempt. Equally important is a broad understanding of the numerous other risk factors that must be assessed in an evaluation of craniopagus twins for separation. As we have discussed in other publications,16 some of the factors critical to the surgical decision making are an understanding of the degree of shared scalp, calvaria, and dura (independent dural envelopes or incomplete dural separation, also called circumferential sinus lakes), the amount of separation/interdigitation or fusion of cortex or deeper structures, the extent of shared arterial connections/cross-flow and common venous sinuses/drainage, and the presence of paired or separate venous outflow/drainage and ventricular systems.16 We have previously proposed a scheme similar to other neurosurgical risk stratification scales (e.g., the Spetzler-Martin scale for arteriovenous malformations) by which individual cases can be evaluated to determine the surgical risk (▶ Table 21.1).16 Our scheme assigns point values to provide a preliminary understanding of the degree of risk associated with attempted separation; a higher score is indicative of a more difficult separation. Few will debate the benefit or detriment of separation if the surgical risk is low or high, respectively, but the decision becomes more difficult in cases that fall between the extremes; however, this scheme may help with the evaluation.17 Although not fully validated, the proposed grading scale attempts to account for the most critical variables that experience has shown to influence outcome during the perioperative period, in an effort to add objectivity to a very subjective decision. Refinement, application, and validation of the scale will occur as additional cases come to modern neurosurgical evaluation.
| Characteristic | Score |
| Scalp | |
| Minor surface area shared (< 10 cm2) | 1 |
| Major surface area shared (> 10 cm2) | 2 |
| Calvaria | |
| Minor surface area shared (< 10 cm2) | 1 |
| Major surface area shared (> 10 cm2) | 2 |
| Dura mater | |
| Independent dural envelope surrounding cortex | 1 |
| Dura shared along one or more planes | 2 |
| Neural tissue | |
| Completely separate | 1 |
| Interdigitated but not fused | 2 |
| Minor areas of fusion (total surface area < 5 cm2) | 3 |
| Major areas of fusion or involvement of eloquent cortex (total surface area > 5 cm2) | 4 |
| Arterial connections | |
| None | 1 |
| Minor feeding branches (M4, A4, P4) | 2 |
| Distal branches (M3, A3, P3) | 3 |
| Proximal branches (M2, A2, P2) | 4 |
| Major vascular trunks (M1, A1, P1, ICA) | 5 |
| Venous connections | |
| None | 1 |
| Separation of major sinuses with minor shared draining veins | 2 |
| Shared along anterior one-third of superior sagittal sinus | 3 |
| Shared distally (transverse/sigmoid) | |
| Shared along posterior two-thirds of superior sagittal sinus without involvement of the torcular | 4 |
| Shared along posterior two-thirds of superior sagittal sinus with involvement of the torcular | 5 |
| Deep venous drainage | |
| Present | 1 |
| Absent | 2 |
| Cerebrospinal fluid (ventricular anatomy) | |
| Separate ventricular systems | 1 |
| Shared ventricular system | 2 |
| Venous outflow | |
| Ipsilateral | 1 |
| Contralateral (crossed) | 2 |
| Arterial flow | |
| Ipsilateral | 1 |
| Contralateral (crossed) | 2 |
| Abbreviations: A, anterior (cerebral artery); ICA, internal carotid artery; M, middle (cerebral artery); P, posterior (cerebral artery). Note: A higher score equates with more difficult separation. Minimum score, 10; maximum score, 28. Source: Reproduced from Browd SR, Goodrich JT, Walker ML. Craniopagus twins. J Neurosurg Pediatrics 1:1–20, 2008.16 | |
21.4 Preoperative Assessment
Understanding and planning for the unique anatomy present in craniopagus is one of the most important factors that lead to a successful separation attempt. Equally important, a high-quality preoperative evaluation can determine which patients are truly inoperable. In the current state, preoperative evaluation consists of clinical monitoring, imaging, and anatomical modeling. Beyond the typical neurosurgical considerations are unique physiologic perturbations that occur in craniopagus that mandate cardiac, pulmonary, and renal management plans. These children often arrive in both cardiac and renal failure and can be severely ill. It has been our experience that the metabolic differences (renal, cardiac, pulmonary, other) between the twins can be quite extreme. These systems and their function can and will change during the perioperative period, and an experienced multidisciplinary medical team is necessary to take these patients up to and through a surgical separation safely. Given the complexity of the procedures and the potential for blood loss with each operation, separations must be delayed until after the patients reach an age and body weight that will allow them to tolerate significant blood loss.
Our ability to obtain high-resolution imaging and newer techniques for modeling blood flow have revolutionized the assessment of craniopagus twins. The reconstruction of high-resolution imaging accurately demonstrates critical neural and vascular structures. Post-processing of these data sets also allows detailed anatomical models to be built of the vascular and cranial structures, aiding in preoperative planning.18 Our focus in early and later imaging series is to understand principally the venous anatomy, as this is often the most challenging issue and early imaging can help determine if separation is even plausible. Computed tomography (CT) and magnetic resonance (MR) imaging will provide a preliminary understanding of the extent of fusion and the complexity of the shared arterial and venous architecture. With this imaging, we can proceed with more complex computer three-dimensional modeling as we transition from evaluation to the surgical planning phase.
Within the last several years, technology has afforded the ability to create detailed three-dimensional anatomical models sourced from DICOM (Digital Imaging and Communications in Medicine) data (▶ Fig. 21.5). Helical CT scanners can obtain high-resolution angiography that is comparable to traditional digital subtraction angiography, with these images converted to three-dimensional computer models for evaluation. The anatomical models can be customized to isolate particular anatomical features one might wish to study, such as the venous anatomy. High-resolution digital reconstructions of CT imaging combined with the three-dimensional models can help with assessment of the degree and orientation of bony fusion. This information is used in planning the surgical corridor, site of separation, and post-separation reconstruction of the cranial vault.

Fig. 21.5 Three-dimensional model based on computed tomographic and magnetic resonance imaging data of craniopagus twins separated at Montefiore.
(Reproduced from Medical Modeling, Golden, CO, and from Douglas Cochrane, MD.)




