“Cystic-Appearing” Posterior Fossa Lesion
Susan I. Blaser, MD, FRCPC
DIFFERENTIAL DIAGNOSIS
Common
Mega Cisterna Magna
Arachnoid Cyst
Dandy-Walker Continuum
Pilocytic Astrocytoma
Encephaloceles
Obstructive Hydrocephalus
Less Common
Epidermoid Cyst
Dermoid Cyst
Neuroglial Cyst
Ependymal Cyst
Hemangioblastoma
Schwannoma (Cystic)
Abscess
Enlarged Perivascular Spaces
Rare but Important
Syringobulbia
Neurenteric Cyst
Atypical Teratoid-Rhabdoid Tumor
Metastases, Intracranial, Other
Neurocysticercosis
Chordoma
Congenital Muscular Dystrophy
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Cystic-appearing lesion exactly like CSF on all sequences?
Mega cisterna magna (MCM), arachnoid cyst (AC), Dandy-Walker Continuum (DW)
Trapped 4th ventricle, enlarged perivascular spaces (↑ PVSs), neuroglial or ependymal cyst
Cystic-appearing lesion not exactly like CSF?
Congenital inclusion cyst (dermoid, epidermoid, neurenteric cysts)
Infection such as abscess, neurocysticercosis (NCC)
Neoplasm (pilocytic astrocytoma, hemangioblastoma, metastasis, chordoma)
Is cyst intra- or extra-axial?
Intra-axial
Trapped fourth ventricle (4th V), ↑ PVSs
Neoplasm (e.g., pilocytic astrocytoma), infection (abscess, NCC)
Inclusion cyst in 4th V (epidermoid)
Extra-axial
MCM, AC, DW, neurenteric cyst, NCC, neoplasm (schwannoma)
DWI, T1 C+ scans helpful additions
Helpful Clues for Common Diagnoses
Mega Cisterna Magna
Communicates freely with all CSF spaces
Normal tegmento-vermian angle (< 5-10°)
Arachnoid Cyst
Mass effect on vermis
± Hydrocephalus
Use FLAIR, DWI to exclude epidermoid
Dandy-Walker Continuum
“Classic” Dandy-Walker malformation
Cystic dilatation 4th V ⇒ ↑ posterior fossa (PF), torcular-lambdoid inversion
Hypoplastic vermis
Vermian remnant rotated anterosuperiorly over cyst
Blake pouch cyst (BPC)
Embryonic BPC doesn’t regress
Enlarged PF, 4th V open inferiorly
Vermis anatomically complete
Pilocytic Astrocytoma
Cystic cerebellar mass
Enhancing mural nodule
Encephaloceles
Isolated encephalocele: Lacks Chiari 2
Chiari 3 = Chiari 2 PLUS
Occipital or cervical encephalocele containing cerebellum
Syndromic occipital encephalocele
Klippel-Feil, Meckel-Gruber, etc.
Obstructive Hydrocephalus
Outlets obstructed→ 4th ventricle ↑ ↑
Maintains “kidney bean” configuration
3rd V, shunted lateral ventricles small
Helpful Clues for Less Common Diagnoses
Epidermoid Cyst
Cerebellopontine angle > 4th V > diploic
Frond-like, cystic (CSF-like)
Doesn’t suppress completely on FLAIR
Restricts on DWI
Dermoid Cyst
Midline “fatty” mass
“Droplets” in CSF if ruptured
Look for dermal sinus, midline vertebral/skull base anomalies
Neuroglial Cyst
CSF-like parenchymal cyst
No enhancement, DWI restriction
Ependymal Cyst
CSF-like
Intra- > paraventricular
Hemangioblastoma
Posterior fossa mass with cyst, enhancing mural nodule that abuts pia
± Arterial feeders, flow-voids
Look for markers of von Hippel-Lindau (VHL)
Visceral cysts, renal clear cell carcinoma
Adult > > older teen (unless VHL)
Check family history!
Schwannoma (Cystic)
Vestibular schwannoma (VS) looks like “ice cream on cone”
Cysts can be intratumoral or VS-associated (arachnoid)
Solid component enhances
Abscess
T2 hypointense rim with surrounding edema
Ring-enhancing
DWI hyperintense, ADC hypointense
Enlarged Perivascular Spaces
CSF-like, nonenhancing, nonrestricting
Most common PF site = dentate nuclei
Less common = cerebellum, pons
Helpful Clues for Rare Diagnoses
Syringobulbia
May occur with either Chiari 1 or 2
Cervical/holocord syrinx common
May extend further into brain (syringocephaly)
Neurenteric Cyst
Slightly hyperintense extra-axial cystic mass, nonenhancing
Anterior pontomedullary, CPA cisterns
Atypical Teratoid-Rhabdoid Tumor
50% infratentorial (usually off-midline)
Intratumoral cysts, hemorrhage common
Gross macrocysts less common
Metastases, Intracranial, Other
Myriad of nonenhancing interfoliate cysts
Low or high grade brain or spine primary
Also reported with breast primary
Choroid plexus papilloma cysts can be entirely extra-axial, nonenhancing
Neurocysticercosis
Cyst with “dot” (scolex) inside
Subarachnoid spaces, sulcal depths most common
Intraventricular cysts often isolated
4th ventricle most common
Chordoma
High signal T2
Moderate to marked enhancement unless necrotic, mucinous
High attenuation foci (CT) may be occult on MR
Congenital Muscular Dystrophy
Best diagnostic clues
Severely “floppy” infant
Z-shaped or cleft pons
Multiple small CSF-like cerebellar cysts (may be PVSs or trapped CSF from overmigration of neurons)
Image Gallery
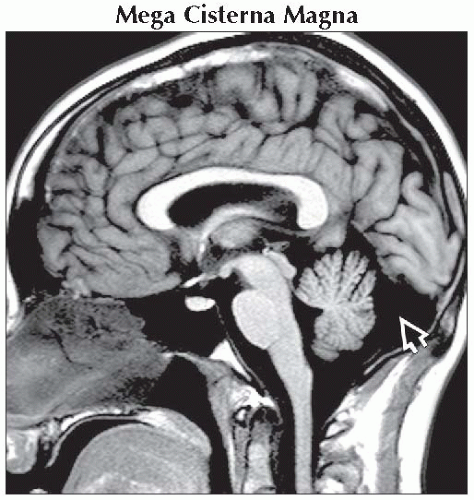 Sagittal T1WI MR shows a mega cisterna magna  . The tentorium is normally located, and the posterior fossa is mildly prominent. There is no mass effect upon the vermis. . The tentorium is normally located, and the posterior fossa is mildly prominent. There is no mass effect upon the vermis. |
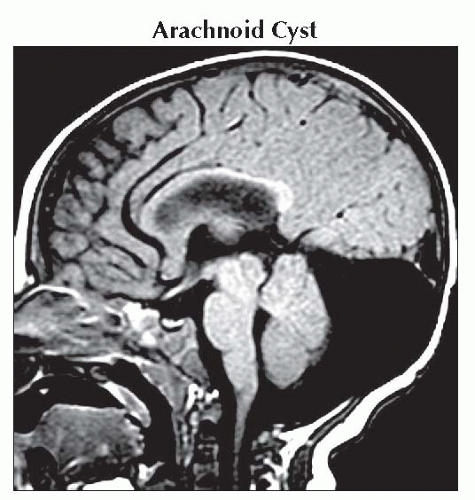 Sagittal T1WI MR shows a retrocerebellar arachnoid cyst. There is enlargement of the posterior fossa, elevation of the tent, and mild compression of the vermis. |
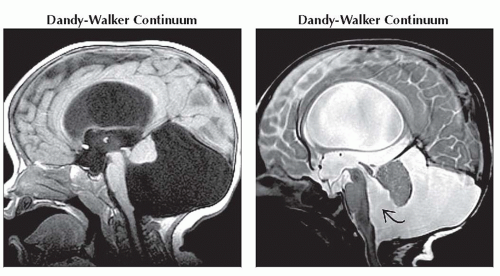 (Left) Sagittal T1WI MR shows typical enlarged posterior fossa, upward rotation of the small vermian remnant, elevation of the tentorium, and mass effect upon the brainstem in “classic” Dandy-Walker malformation. (Right) Sagittal T2WI MR shows enlargement of the inferior 4th ventricle
 , which communicates with an enlarged cisterna magna in this infant with a Blake pouch cyst. , which communicates with an enlarged cisterna magna in this infant with a Blake pouch cyst.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|