Differential Diagnosis of the Cervical Spine: Spinal Masqueraders
Differential Diagnosis of the Cervical Spine: Spinal Masqueraders
Ricky James Placide
A multitude of pathologic conditions can affect the structure and function of the cervical spine, contributing to a variety of signs and symptoms. These conditions can be categorized as degenerative, traumatic, infectious, neoplastic, congenital, inflammatory, autoimmune, and vascular. Obtaining an accurate patient history, complete physical examination, and appropriate imaging studies will typically lead the clinician to the appropriate diagnosis. There are, however, medical conditions with signs and symptoms similar to those due to cervical spine disease, but the actual problem stems from a disease or condition other than the cervical spine. In these cases, presenting signs and symptoms mimic a cervical spine problem, often misleading even the most astute clinician. These nonspine conditions with “spine-like” signs and symptoms are referred to as spinal masqueraders (1).
Essentially any body system can produce signs and/or symptoms that can masquerade as cervical spine pathology, some of which are relatively benign; others can be life threatening. Masquerading symptoms can be in the form of axial neck pain and/or radiculopathy/myelopathy. In the context of differential diagnosis, three main scenarios exist. For example, if a patient appears to have a cervical radiculopathy, the patients’ signs and symptoms can be due to (a) a cervical radiculopathy, (b) a spinal masquerader, or (c) a combination of both a cervical radiculopathy and a masquerader. This method of evaluation can be applied across the formulation of a differential diagnosis for any set of signs and symptoms.
This chapter reviews some cervical spine masqueraders in the context of the organ system with which they are associated, including the musculoskeletal, neurologic, cardiovascular, and visceral organ systems. There are many less commonly encountered conditions that can mimic cervical spine disease, and this chapter, while not all inclusive, will serve as an introduction to the topic of spinal masqueraders.
MUSCULOSKELETAL SYSTEM
Many conditions of the musculoskeletal system have been shown to mimic cervical spine disease by producing axial pain and/or pseudoradicular pain (2, 3 and 4) (Table 11.1). The majority of these conditions can be differentiated from cervical spine disease by a careful history and physical examination. Some are due to a local inflammatory state such as rotator cuff tendinitis, while others are due to a systemic inflammatory condition, such as polymyalgia rheumatica (PMR).
Of all the musculoskeletal conditions of the upper extremity that can mimic cervical spine disease, the tendinopathies are the most common. These include rotator cuff tendinitis, medial and lateral epicondylitis, and wrist flexor and extensor tendinopathies such as DeQuervain’s tenosynovitis. A careful history and physical examination should allow the clinician to differentiate these musculoskeletal conditions from cervical radiculopathy. While these conditions can refer pain a distance from the local site of pathology, the reference pattern should not be in a dermatomal pattern. Any weakness will likely be pain related (excluding a tendon rupture) and not in a myotomal pattern. In the case of a tendinitis, there is typically palpable tenderness, not usually a feature of radiculopathy. Rotator cuff tendon pathology, being the most common upper extremity musculoskeletal pathology to masquerade as a cervical spine condition, will be discussed in more detail.
When evaluating the patient with suspected cervical radiculopathy, shoulder pathology needs to be in the differential diagnosis and may present as the primary problem or as a coexisting condition with cervical spine disease. Recall that the term “shoulder” refers to a system including four separate articulations (glenohumeral, scapulothoracic, acromioclavicular, and sternoclavicular joints), multiple ligaments, a variety of muscles, and complex biomechanical functioning. While a detailed review of shoulder function is beyond the scope of this chapter, the more common conditions mimicking cervical spine disease can be simplified to the rotator cuff and associated pathology.
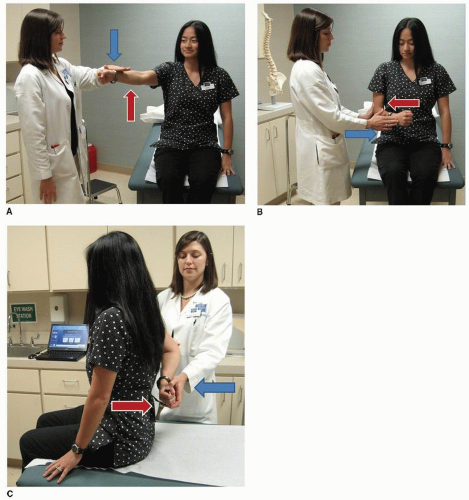
The rotator cuff is a group of four muscles important for proper functioning of the shoulder complex. The four muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. They all receive innervation from spinal levels C5 and C6; however, their peripheral nerve innervations vary. The supraspinatus and infraspinatus are innervated by the suprascapular nerve, the teres minor by the axillary nerve, and subscapularis by the upper and lower subscapular nerves. Figure 11.1 demonstrates the method for evaluating the competence of the rotator cuff musculature.
TABLE 11.1 Musculoskeletal Conditions Known to Mimic Cervical Spine Disease
Temporomandibular joint dysfunction
Costochondritis
Shoulder
Rotator cuff tendinitis/tear
Osteoarthritis
Adhesive capsulitis
Bursitis (subacromial, scapulothoracic)
Elbow
Lateral epicondylitis
Medial epicondylitis
Bursitis (olecranon)
Wrist/Hand
Flexor tendinitis
Extensor tendinitis
DeQuervain’s tenosynovitis
Systemic conditions
MFPSs and dysfunction
When differentiating shoulder from cervical spine pathology, it is not as important initially to differentiate between individual shoulder conditions, as many of them have similar signs and symptoms. For the purposes of this discussion, shoulder pathology will mean most intrinsic glenohumeral joint conditions, the more common being rotator cuff tendinitis/tear, glenohumeral arthritis, impingement syndrome, adhesive capsulitis, and subacromial bursitis.
Shoulder pathology will most commonly mimic a C5 radiculopathy, but C4 and C6 will be in the differential. Shoulder pathology can refer pain from the nape of the neck to the level of the elbow. Shoulder pain does not typically refer distal to the elbow. Many signs and symptoms of shoulder pathology and cervical radiculopathy are the same; however, a careful history and physical examination will usually differentiate between these two conditions. Remember, it is not uncommon for shoulder pathology and cervical radiculopathy to coexist.
The patient with shoulder pathology will usually complain of activity-related pain, typically with overhead activities, whereas someone with a cervical radiculopathy may find placing the arm overhead relieves the pain. This is because lifting the arm overhead increases impingement of the rotator cuff (supraspinatus) and decreases neural tension (5). The primary region of pain with shoulder pathology is centered about the shoulder itself, typically superolaterally, with referred pain to the level of the deltoid tuberosity. Shoulder pathology normally does not refer pain distal to the elbow unlike cervical radiculopathies C6-T1, which often have symptoms distal to the elbow. Note that intrinsic shoulder pathology can lead to neck and periscapular pain due to faulty glenohumeral mechanics and neuromotor compensation. In the case of shoulder pathology, particularly a rotator cuff tear, the patient will complain of night pain and the inability to lie on the involved side.
While a patient history cannot always give the clinician the diagnosis, it can help narrow the differential. The physical exam will help narrow the differential even more. In the case of shoulder pathology, neurologic findings such as dermatomal sensory disturbances, myotomal weakness, and changes in deep tendon reflexes should be absent. The clinician must differentiate spinal level motor weakness from that of intrinsic shoulder muscle weakness (Fig. 11.1). This will be more difficult in the case of painrelated weakness. Keep in mind peripheral neuropathies that can mimic both shoulder and cervical spine diseases such as a suprascapular neuropathy due to a glenoid cyst (see section on peripheral neuropathy).
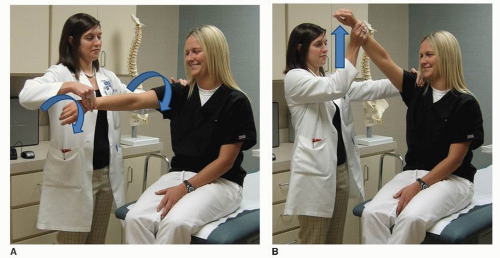
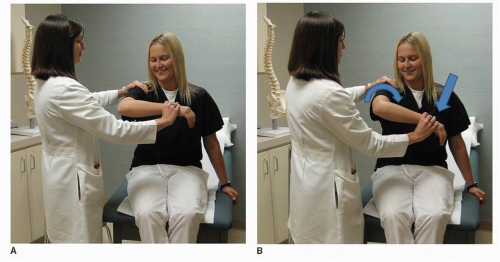
In addition to the dermatome, myotome, and reflex examination, several other provocative exam maneuvers will help to differentiate shoulder from cervical spine pathology. Spurling’s maneuver is designed to reproduce symptoms of a cervical radiculopathy by decreasing the neuroforaminal space in an already pathologic spinal level (6). This test should not reproduce symptoms related to shoulder pathology. Neer’s impingement test and Hawkins’ sign are physical exam maneuvers designed to reproduce symptoms of rotator cuff pathology (and most intrinsic shoulder pathology) (Figs. 11.2 and 11.3). These tests will cause compression of the rotator cuff beneath the coracoacromial arch, eliciting pain. These tests should not provoke symptoms of cervical radiculopathy.
After the history and physical exam, the next step in the evaluation process may include imaging studies. Plain radiographs, computed tomography, and magnetic resonance imaging all play a role and can be confirmatory in many cases. Realize there are also many false-positive findings on imaging studies, and without a history and physical, imaging can be quite misleading (7,8). Additionally, electromyography (EMG) and nerve conduction velocity (NCV) testing are occasionally helpful, especially in the case of coexisting pathologies.
NEUROLOGIC SYSTEM
Many nonspine conditions of the neurologic system will mimic cervical axial pain, radiculopathy, and myelopathy. While most will be a peripheral neuropathy of some sort, intracranial processes will also present with signs and symptoms of cervical spine disease. For example, cases of spontaneous intracranial hypotension, normal pressure hydrocephalus, intracranial neoplasm, Chiari malformation, migraine headache, multiple sclerosis, and cerebrovascular accident have all been reported with presenting signs and symptoms consistent with cervical spine disease (9, 10, 11, 12, 13 and 14). Usually, a careful history, physical examination, and occasionally time, will lead the clinician down the correct diagnostic pathway.
By far the most common nervous system condition to mimic cervical spine pathology is peripheral neuropathy. The clinical presentation of peripheral nervous system pathology is commonly confused with cervical radiculopathy and myelopathy. This chapter divides peripheral neuropathies into compressive and noncompressive etiologies and will discuss the more common compressive neuropathies. As for the noncompressive neuropathies, the differential is exhausting, and a partial list is shown in Table 11.2. Since most of the noncompressive conditions are systemic in nature, the neuropathy can affect the upper and/or lower extremities, thereby mimicking cervical myelopathy and radiculopathy. Remember that patients with, for example, diabetes, are at risk for peripheral polyneuropathy due to their disease, but they are also at increased risk of developing compressive mononeuropathies.
Figure 11.1. Testing of the rotator cuff muscles in the position of maximal electrical activity. A: Supraspinatus (abduction). B: Infraspinatus (external rotation) and teres minor. C: Subscapularis (internal rotation).
One of the primary concern during the initial assessment process is the differentiation between a spine and a peripheral etiology. This can be accomplished by appreciating the occasionally subtle differences between spinal level innervations (dermatomes and myotomes) and peripheral nerve innervations. For example, the C6 dermatome overlaps with peripheral nerve sensory innervations from the lateral antebrachial cutaneous nerve, the superficial radial nerve, and the median nerve. The following section will discuss brachial plexopathy and suprascapular neuropathy due to their often complex presentation and differential diagnosis, which includes cervical radiculopathy, rotator cuff disease, compressive peripheral neuropathy, and noncompressive neuritis. This section will then conclude with a discussion of the common compression neuropathy syndromes of the upper extremity involving the three major upper extremity peripheral nerves: the median, ulnar, and radial nerves. A more comprehensive list is presented in Table 11.3.
Figure 11.2. Neer’s impingement test. The shoulder is placed in 90 degrees of flexion, 45 degrees of horizontal abduction and internal rotation, then the shoulder is flexed. A: Starting position. B: Ending position.
BRACHIAL PLEXOPATHY AND NEUROGENIC THORACIC OUTLET SYNDROME
Disorders of the brachial plexus can be extremely varied and are likely a reflection of the complex neuroanatomy, as well as the surrounding anatomy and susceptibility to injury. Etiologies include acute traumatic injury (compression, traction), chronic compressive pathology, infectious disease, inflammatory conditions, and idiopathic causes (15,16). The following section focuses on compressive pathology of the brachial plexus and thoracic outlet syndrome (TOS).
Figure 11.3. Hawkins’ impingement test. The shoulder is placed in 90 degrees of flexion, staying in the sagittal plane, and the shoulder is internally rotated. A: Starting position. B: Ending position.
TOS is a complex condition. The distinction needs to be made between neurogenic thoracic outlet syndrome (nTOS), arterial thoracic outlet syndrome (aTOS), and venous thoracic outlet syndrome (vTOS) (15). The latter two will be discussed in the cardiovascular section. Greater than 90% of the cases of TOS are the neurogenic type (15,16). While the brachial plexus can be compressed anywhere along its course, there are three principle locations where the likelihood is increased. The first is the so-called scalene triangle where the brachial plexus (and subclavian artery) pass between the anterior and middle scalene muscles. The second passage is through the costoclavicular space, between the clavicle and the first rib. Finally, the brachial plexus courses beneath the coracoid process, through the subcoracoid tunnel.
TABLE 11.2 Selected Pathologic Conditions Associated with Noncompressive Peripheral Neuropathy
Hereditary neuropathies
Hereditary sensorimotor neuropathy
Hereditary sensory neuropathy
Metabolic neuropathies
Diabetes
Amyloidosis
Hypothyroidism
Uremia
Acute intermittent porphyria
Nutritional neuropathies
Pyridoxine (B6) and cobalamin (B12) deficiency
Combined subacute system degeneration
Alcoholism
Autoimmune neuropathies
Systemic lupus erythematosus
Sarcoidosis
Polyarteritis nodosa
Sjogren’s disease
Neoplastic neuropathies
Paraneoplastic syndromes
Infectious neuropathies
Lyme’s disease
Herpes zoster
Diphtheria
Guillain-Barre syndrome
Toxic neuropathies
Arsenic
Lead
Isoniazid
Cisplatin
Organic solvents
Idiopathic neuropathies
Brachial neuritis (Parsonage-Turner syndrome)
Only gold members can continue reading. Log In or Register to continue
 Developmental Anatomy of the Normal Cervical Spine
Developmental Anatomy of the Normal Cervical Spine
 Cervical Radiculopathy: Diagnosis and Differential Diagnosis
Cervical Radiculopathy: Diagnosis and Differential Diagnosis
 Cervical Spine Injuries in Children
Cervical Spine Injuries in Children
 Calcification of the Ligamentum Flavum of the Cervical Spine
Calcification of the Ligamentum Flavum of the Cervical Spine
 Artificial Disk Surgery of the Cervical Spine: Contraindications for Cervical Disk Arthroplasty
Artificial Disk Surgery of the Cervical Spine: Contraindications for Cervical Disk Arthroplasty
 Controversies, Myths, and Realities Regarding the Surgical Treatment of Cervical Spondylotic Myelopathy with a Special Focus on Laminoplasty
Controversies, Myths, and Realities Regarding the Surgical Treatment of Cervical Spondylotic Myelopathy with a Special Focus on Laminoplasty



